

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The coccyx, or tailbone, is the most distal segment of the spine. Although the coccyx is a rudimentary structure, the levator ani, iliococcygeus muscle, and several ligaments are attached to the structure. These muscle and ligament structures support the pelvic floor and contribute to voluntary movement.
Pain can develop around the coccyx, which is referred to as coccydynia or coccygodynia. Numerous studies have suggested the causes of the pain.123456789101112) Coccydynia can result from external trauma; repetitive minor trauma such as prolonged sitting on hard, uncomfortable surfaces; and internal trauma during childbirth.123456789101112) Other causes such as local tumor, inflammation, disc degeneration, and idiopathy, have also been proposed. It is well known that females have a 4 to 5 times higher incidences of coccydynia than men.10) Although the cause of the higher incidences of coccydynia in females has not been elucidated, most authors attributed it to differences in the morphology and mobility of the sacrococcygeal segments between males and females.613141516)
Postacchini and Massobrio5) suggested a radiologic classification of the coccyx and described the relationship between the coccygeal type and pain. There have been several articles on the morphology and morphometry of the sacrococcygeal region in Arabs and Europeans using computed tomography (CT) or magnetic resonance imaging (MRI).131415) However, to the best of our knowledge, there has been no previous study on the coccygeal morphology in Asian ethnicities. In this study, we investigated the morphology and morphometry of sacrococcygeal anatomy of Koreans using CT and compared morphologic differences among ethnic groups.
METHODS
This study was conducted on patients who had a pelvic or sacral CT in a single hospital between 2008 and 2014. Patients with a sacral fracture, a coccyx fracture, or a deformed sacrum due to tumor or infection were excluded. A total of 606 CT scans were available for the analysis. A 128-slice multidetector CT scanner (iCT 128 scanner; Philips, Cleveland, OH, USA) was used for the study. Digital images of the lumbosacral junction and the whole coccyx were obtained with the PACS system (STARPACS5081; INFINITT Healthcare, Seoul, Korea). CT was taken with all patients in the supine position.
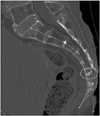
The qualitative and quantitative parameters of the sacrococcygeal anatomy were assessed. The definitions of these parameters are presented in Table 1.131415) The type of coccyx was determined based on the classification proposed by Postacchini and Massobrio.5) Their classification was modified on the basis of the angle between a line drawn from the first coccygeal segment to the tip of the last coccygeal segment and a vertical line on the CT scan referring to the horizontal line of the supine position. If the angle was larger than 30°, the coccyx type was type II; if it was less than 30°, the coccyx type was type I. The morphological parameters were sacrococcygeal fusion, the coccygeal segmental number, and the coccygeal type (Fig. 1). The morphometric parameters were the sacral and coccygeal curved indexes and the sacrococcygeal and intercoccygeal angles (Table 1 and Fig. 2). The age- and gender-matched differences of these parameters were analyzed. Cases with sacrococcygeal fusion cases, those parameters were not assessed to avoid confusing the sacrococcygeal junction's location. Sacrococcygeal fusion was defined as continuation of the anterior and posterior cortices between the sacrum and the coccyx. However, there could be the possibility of sacralization of the first coccygeal segment. Since it was not feasible to differentiate sacrococcygeal fusion from sacralization of the first coccygeal segment, sacralization cases were also considered as sacrococcygeal fusion cases.
Two orthopedic surgeons measured the parameters twice, with a 2-week interval between measurements. Averages of the parameters were used for statistical analysis.
Statistical Analysis
Data analysis was performed using SPSS ver. 19 (IBM Co., Armonk, NY, USA). The most common type of coccyx, the number of coccygeal segments, the average of the sacral and coccygeal curved indexes, and the sacrococcygeal and intercoccygeal angles of Koreans were assessed. The correlation between the sacral curved index and age (stratified by decade) was analyzed using Spearman correlation. The correlations of the coccygeal curved index, sacrococcygeal angle, and intercoccygeal angle among patients in each decade of life were analyzed using the same method. Spearman correlation coefficient (r) was interpreted as poor if < 30, fair if 0.31–0.50, moderate if 0.51–0.60, moderately strong if 0.61–0.80, and very strong if > 0.80. The differences in the sacrococcygeal morphometry between males and females were analyzed using an independent t-test. The sacrococcygeal fusion rate, the number of coccygeal segments, and coccygeal type according to the decade of age were analyzed using linearby-linear association. The difference in the sacrococcygeal fusion rate between males and females was analyzed using a chi-square test.
An intraclass correlation coefficient (ICC) was calculated to assess the intraobserver and interobserver reliability. The reliability was determined by repeating the measurements in 30 subjects two weeks after the initial measurement, using CT scans. A p-value less than 0.05 was considered statistically significant.
This study was approved by the Institutional Review Board of the Cheju Halla General Hospital.
RESULTS
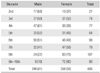
A total of 248 males (40.9%) and 358 females (59.1%) were included in this study. The average age of the subjects was 55.5 years (range, 16 to 97 years). The number of subjects in each age group stratified by decade of life was 27 in the second, 74 in the third, 77 in the fourth, 64 in the fifth, 98 in the sixth, 79 in the seventh, 107 in the eighth, and 80 in the ninth and tenth decades of life (Table 2).
Coccygeal Morphology
The most common type of coccyx among Korean patients was type II (51%), followed by type I (27.4%). Types III, IV, and V were 14.7%, 4.5%, and 0.2%, respectively. There was no significant difference in the coccygeal type between males and females (p = 0.126). However, the rate of type II compared with other types was significantly higher in females than males (54.7% vs. 45.6%, p = 0.032) (Table 3). The coccygeal type was significantly different among the age groups (p = 0.015): the type I ratio increased in the eighth-decade (29.9%) and ninth and tenth decades (40%) compared with the averages in the other decades (27.4%) (Table 4). The numbers of coccygeal segments were not significantly different between gender (p = 0.231) (Table 3). However, there was a weak negative correlation between the number of coccygeal segments and the age (r = −0.112, p = 0.007) (Table 4). Four coccygeal segments were the most common and present in 379 of individuals (64.8%), followed by three segments in 169 (28.9%).
The sacrococcygeal fusion rate significantly increased in the eighth (38.3%) and ninth and tenth (46.3%) decades compared with the other decades (average, 33.4%; p = 0.02) (Table 4). The sacrococcygeal fusion rate was not significantly different between genders, except in the ninth and tenth decades (p = 0.283) (Tables 3 and 4). These subjects were excluded from the analysis due to the very small number of males (8) compared with females (71).
Coccygeal Morphometry
The mean straight lengths of the coccyx and sacrum were 34.7 mm and 108.3 mm, respectively, while the mean curved lengths were 37.6 mm and 115.3 mm, respectively. The mean curved indexes of the coccyx and sacrum were 7.41 and 6.15, respectively. The average sacrococcygeal and intercoccygeal angles were 110° and 49°, respectively. The curved index of the sacrum increased with age, showing a fair positive correlation (r = 0.493, p = 0.000), while the curved index of the coccyx decreased with age, showing a weak negative correlation (r = −0.257, p = 0.000). As the age increased, the sacrococcygeal angle increased, showing a weak positive correlation (r = 0.21, p = 0.000), while the intercoccygeal angle decreased, showing a weak negative correlation (r = −1.87, p = 0.000). As the age increased, the sacral curved index became larger and the sacrococcygeal angle increased, while the coccygeal curved index and intercoccygeal angle decreased (Table 5 and Fig. 3). There were significant differences in the curved indexes of the coccyx and sacrum between genders. The mean coccygeal curved index was larger in males (8.89) than females (6.26, p = 0.000), while the mean sacral curved index was smaller in males (5.28) than females (6.83, p = 0.000). The mean sacrococcygeal angle was not significantly different between genders (p = 0.201), while the mean intercoccygeal angle was significantly larger in males than females (53.9° vs. 44.7°, p = 0.000). These results indicate that the coccyx was more curved and the sacrum was straighter in males than females (Table 5 and Fig. 4).
DISCUSSION
To the best of our knowledge, this study is the first to investigate the morphology and morphometry of the sacrococcygeal anatomy of Koreans and other Asians using CT. The most frequent number of coccygeal segments of Arabs was three13) while that of Europeans was four.1415) In our study, four coccygeal segments were most common (64.8%). This difference in the number of coccygeal segments among ethnicities might be due to intercoccygeal or sacrococcygeal fusion. In this study, although sacrococcygeal fusion cases were excluded from the analysis, fusion of the third and fourth segments of the coccyx might have caused reduction in the number of segments. Occasional fusion of the second and third segments of the coccyx was also noted. The number of coccygeal segments might have been decreased due to the aging-related fusion of the intercoccygeal segment. The most common type of coccyx in this study was type II (51%) followed by type I (27.4%). In Arabs and Europeans, except for one study,17) type I coccyx was most common, followed by type II. This might be due to the fact that there are some ambiguous features in the classification of Postacchini and Massobrio,5) especially between types I and II. For classification, we measured the angle created by a line drawn from the first coccygeal segment to the tip of the last coccygeal segment and a vertical line. The tip of the type I coccyx directed more downward. According to previous literature, types III and IV were more common in males, whereas there was no significant difference in the coccygeal type between genders in our study. However, type II was more common in females, and the tip of the coccyx directed more ventrally than in males as in other studies.131415) There was a significant difference in the coccygeal type among age groups in this study. Older patients (those in the eighth, ninth, or tenth decades) were more likely to have type I coccyxes, indicating a more downward position of the coccyx, than those in the seventh decade. Korean patients had similar coccyxes as those of Arabs.13)
The average fusion rate of the sacrococcygeal joint was 33.4%, similar to that of other studies.13141518) Fusion of the sacrococcygeal joint was more common in older patients, especially those in the eighth, ninth or tenth decades, while there was no significant difference between males and females. For comparative study with regard to gender, the patients in the ninth and tenth decades were excluded due to the very small number of males. Some authors claimed that fusions are observed more frequently in elderly females1920) or occur later in women.21) Some authors, however, insisted that the incidence of sacrococcygeal fusion is not simply a reflection of age or sex.22) In our study, although gender was not an influencing factor, but age appeared to affect fusion rates. Older patients had sacrococcygeal fusion more frequently.
The straight and curved lengths of the sacrum and coccyx in males were larger than those in females. These results are similar to data in the literature.131415) However, the curved indexes of the sacrum and coccyx between males and females are controversial. In this study, females had straighter coccyxes and more curved sacrums than males. These findings are similar to those in Europeans,141523) but different from those in Arabs.13) There was no significant difference in the sacrococcygeal angle between genders, while the intercoccygeal angle was larger in males. The difference of the intercoccygeal angle between genders was also similar to Europeans, but different from Arabs. The coccyx of Arabs was more curved, with a larger intercoccygeal angle in females, suggesting that the anatomical features of females might predispose them to a higher risk of developing coccydynia.13) Some authors reported that the intercoccygeal angle was a useful radiological measurement to evaluate the forwardly angulated deformity of the coccyx, and the intercoccygeal angle of the idiopathic coccygodynia group was greater.7) Arabic females had more curved coccyxes and this feature was correlated with the prevalence of coccydynia, whereas in our study and European studies, females had straighter coccyxes and type II (more forwardly directed coccyx) was more common in females (Fig. 3). We could not determine the relationship between the coccygeal morphology (curvature or type) of females and coccygodynia. Several studies have disclosed that hypermobility of the coccygeal segment or a rigid coccyx with a predominant tip might be a possible cause of painful coccyx rather than the morphology.11424) Thus, the controversy on the relationship between coccygeal morphology and coccydynia remains unresolved.
In this study, as age increased, the sacral curved index and the sacrococcygeal angle also increased, while the coccygeal curved index and intercoccygeal angle decreased. The sacrum was more curved and the coccyx was straighter in older patients. Similar results were also found in Arabic coccygeal morphometry; however, this morphologic change was observed among those aged 50 years or older in Arabic subjects,13) whereas it was seen in patients over 70 years of age in Korean subjects.
Although our patient cohort was reasonably large and the methodology was reliable, there are some limitations to this study. The first limitation is that we could not determine the relationship between the anatomical morphology of the sacrococcygeal region and coccydynia. In this study, the subjects were not divided by the presence or absence of coccydynia, and we, therefore, could not assess the prevalence of coccydynia in these subjects. The second limitation was that the CT image was obtained with the patient placed in the supine position. A different coccygeal type may be observed when the patient stands due to a change in the pelvic tilt. However, we studied only the static sacrococcygeal morphology and previous reports also assessed the coccygeal type based on the images obtained in the supine position, which allowed for the comparison with previous studies on the coccygeal type. The third limitation was that CT scans could only show static sacrococcygeal morphology, and thus the mobility of the coccyx could not be evaluated.
The other anatomical features that can lead to coccygeal pain, spicule, subluxation, and ventral curve of the last segment of the sacrum were not analyzed in this study. Other factors, such as body mass index and obesity, could not be included to analyze other anatomical differences that could affect morphology.
In conclusion, we studied the morphology and morphometry of the sacrococcygeal anatomy in 606 Korean patients. Our patients had similarities and differences with other ethnic groups. The most common type of coccyx was type II and the average number of coccygeal segments was four. There were some differences in coccygeal anatomy between genders; females had a more curved sacrum and straighter coccyx than males. Females had type II coccyxes (ventrally forward coccyx) more frequently than males. However, it could not be determined whether the differences in sacrococcygeal anatomy would affect coccydynia that occurs more often in females.
The sacrococcygeal morphology changed with the aging process. When subjects were older, the sacrum tended to be more curved and the coccyx straighter, especially in patients over 70 years of age. In addition, the sacrococcygeal fusion rate increased in patients over 70 years of age. Knowledge of the sacrococcygeal anatomy of Koreans will improve understanding of the anatomical differences between ethnicities and facilitate future studies on coccydynia.







 XML Download
XML Download