

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The humerus can be considered the most versatile bone in the human body in view of the fact that it can be successfully approached by a variety of methods for fracture fixation including functional bracing, plating (posterior, lateral, and anterior), and intramedullary nailing (antegrade and retrograde).12345) Plating can be performed using a classic open approach or minimally invasive methods. Notably, many humeral fractures can be successfully managed conservatively due to the wide range of acceptability for reduction. In the presence of a myriad of treatment options, it is necessary to individualize these options depending on the patient profile.
Anterior bridge plating (ABP) which utilizes the minimally invasive approach popularly known as the minimally invasive percutaneous plate osteosynthesis (MIPPO) technique can be said to be the latest entrant in this list. The recent literature search gives numerous publications pertaining to this topic in a variety of case scenarios.46789) However, to the best of our knowledge, there are no studies exclusively dealing with mid-shaft humerus fractures in patients predominantly involved in overhead activities: i.e., athletes and manual laborers who perform activities that place extra load on the upper limbs.
The traditional open posterior plating is a rotator cuff safe technique; however, biological disruption of soft tissue, poor cosmetic scarring, and direct handling of the radial nerve have been of concern. On the other hand, the classical intramedullary nailing is minimally invasive, but it has the main drawback of potentially damaging the rotator cuff and causing shoulder impingement.1351011) The ABP is designed to combine the best features of these two techniques: therefore, it is minimally invasive and cosmetic friendly and causes minimal manipulation of vital structures.1012131415)
In this study, we investigated the efficacy of ABP in the abovementioned population.
METHODS
For the period from May 2013 to May 2014, a prospective study involving 57 patients who met the inclusion criteria and underwent ABP was performed at the authors' institute (Dr. V. M. Government Medical College & S. C. S. M. General Hospital, Solapur, India). The study design was reviewed and approved by the Departmental & Institutional Ethics and Review Board (ortho/2015/05/01). Informed consent was obtained from all patients for use of their clinical/imaging data and for subsequent follow-up examinations and radiology. All the patients were followed for a minimum of 1 year. Out of the original 57 patients, 5 were lost to follow-up, 3 died due to unrelated causes (2 due to road traffic accidents and 1 due to cardiac arrest), and 1 sustained an ipsilateral forearm fracture after an accident at 6 months after the humeral surgery. These 9 patients were excluded from the final analysis. Consequently, the final patient cohort consisted of 48 patients (follow-up rate, 84.21%).
The inclusion criteria are as follows: (1) mid-shaft humeral fractures; (2) occupation predominantly involving overhead activities: i.e., throwers, athletes, and laborers; (3) skeletally mature; (4) minimum 1-year follow-up at the time of study. The exclusion criteria are as follows: (1) ipsilateral upper limb trauma/neurovascular insult or any other major injuries elsewhere which had the potential to jeopardize the patient rehabilitation; (2) history of old humeral fractures; (3) skeletally immature; (4) history of any systemic diseases severely affecting the bone, any primary bone disease, or malignancy anywhere in the body; and (5) open fractures.
Surgical Technique and Postoperative Rehabilitation
After a routine preanesthetic check-up, patients were sent for submuscular, extraperiosteal anterior humeral bridge plating using a standard technique performed in the supine position under fluoroscopic guidance. The shoulder was abducted to 30°–60°, the elbow was flexed to about 90°, and the forearm was supinated throughout the procedure. Indirect reduction maneuvers were used when needed for optimal fracture reduction. The proximal part of incision was about 2–3 cm long between the deltoid and biceps and as proximal as possible in this intermuscular plane, whereas the distal incision of a similar length was made as distal as possible while ensuring that the plate ended proximal to the supracondylar region, and the brachialis was split to reach the anterior surface of the humerus. The biceps and underlying neurovascular bundle were retracted medially while the lateral part of the split brachialis muscle protected the radial nerve. Undue forceful retraction was avoided for fear of neuropraxia. As described by Wang et al.,15) 15° of angulation in any plane and 1 cm migration of fracture ends were the threshold of acceptability and anything more than that merited a second attempt for reduction. The cortical step sign and diameter difference sign described by Krettek et al.16) were used to minimize malrotation during fixation.
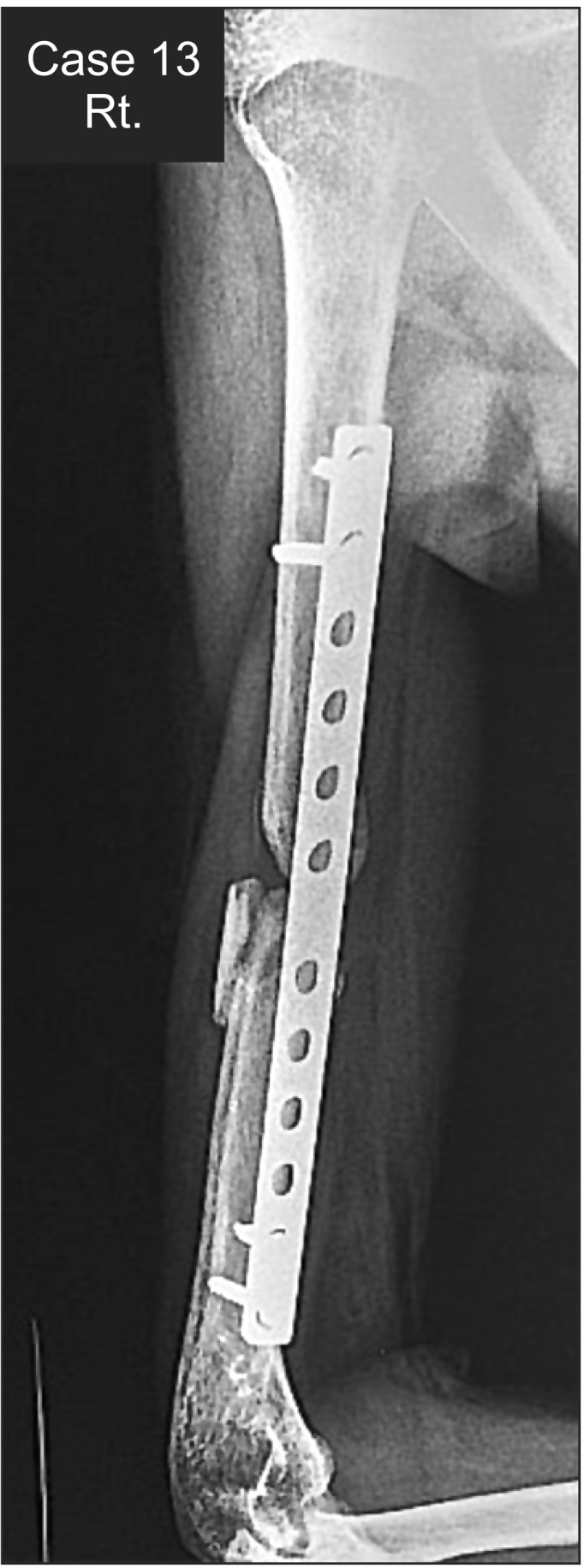
The longest possible 4.5-mm dynamic/locking compression plate (DCP/LCP) was chosen depending on the humeral anatomy. During insertion of the distal screws on the anterior surface (Fig. 1), care was taken to the proximity of the radial nerve laterally and brachial artery and musculocutaneous nerve medially.1217181920) Simple cortical screws were used in all cases (two proximally and two distally) except when the bone was extremely osteoporotic where locking screws were used (Fig. 1).

Postoperatively, all patients were discharged after 48 hours with the affected side immobilized in a simple sling. Pendulum exercises and elbow, wrist, and hand range of motion (ROM) exercises were started immediately postoperatively as tolerated by the patient. Passive and active-assisted shoulder ROM exercises were started under supervision of a physiotherapist at 2 weeks after surgery. Active abduction beyond 90° and active rotation were allowed at 3–4 weeks after surgery. The patient was allowed to gradually resume preoperative activities with muscle strengthening and return to full spectrum of activities at 9–12 weeks after surgery.
Patients with no signs of radiographic/clinical union at more than 180 days or 6 months after surgery were subsequently treated for nonunion.
Assessment of Outcomes
Patients were assessed for functional and radiological outcomes at 1 year after surgery. Two fellowship-trained surgeons performed all the assessments. Serial radiographs were obtained immediately after surgery, at 6 weeks, 3 months, and 6 months after surgery, and finally at 12 months after surgery. The radiographs were re-evaluated with help of a musculoskeletal radiologist who was blinded to this study. Radiographic assessments included callus formation, fracture alignment, delayed union, and nonunion.
The functional outcome was assessed using the Constant score, Mayo's elbow score, and Disabilities of the Arm, Shoulder and Hand (DASH) score. The ROM of the affected limb was evaluated for abduction, external rotation (ER) in 90° of abduction and elbow flexion, internal rotation (IR) with the arm placed adjacent to the chest and elbow flexed to 90°, and forward elevation (FE) using a hand-held goniometer. The strengths of the shoulder abductors, rotators, and forward elevators and elbow flexors and extensors were assessed using the Medical Research Center grading, and side to side difference was calculated as well. These measurements were re-evaluated by a senior physiotherapist who was blinded to this study.
A patient satisfaction questionnaire was administered and the patients were asked to answer at the end of the study. The questionnaire consisted of "yes-no" type questions related to quality of life and sleep; return to activities and performance therein; pain, discomfort, and cosmesis related to the procedure; and finally the likelihood of recommendation of the procedure to others or undergoing it again, if a need arises in the future. The answers were assessed and final patient outcome and satisfaction were graded as poor, fair, good, very good, and excellent.
Statistical Analysis
The data on categorical variables are presented as the number of patients (%) and the data on continuous variables are presented as mean ± standard deviation (SD). The statistical significance of pair-wise difference of the mean of continuous variables was tested using Wilcoxon signed rank test and that of one-sample distribution was tested using one-sample chi-square test for majority. A p-value less than 0.05 was considered statistically significant. All the hypotheses were formulated using two tailed alternatives against each null hypothesis (hypothesis of no difference). The entire data were statistically analyzed using SPSS ver. 11.5 (SPSS Inc., Chicago, IL, USA) for MS Windows.
Go to : 
RESULTS
The demographic profile of the patients is tabulated in Table 1.
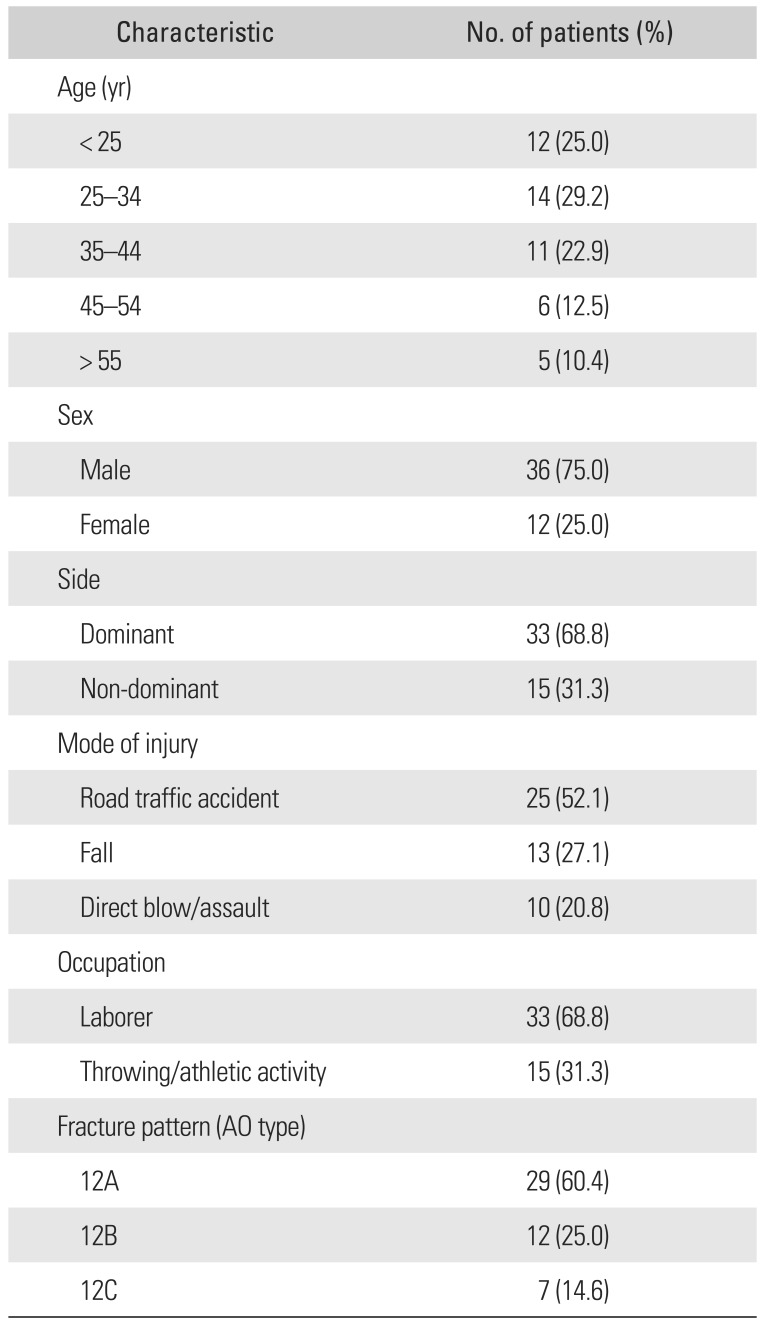
Table 1
The Distribution of General Characteristics of the Patients Operated (n = 48)
![]()
Of the 48 patients assessed, all but two united successfully without additional intervention. These 2 cases (4.17%) of nonunion were treated with autologous iliac crest bone grafting at 6 months after surgery and further recovery was uneventful in both of them, with the fracture uniting 8 weeks afterwards. One of them was a chronic tobacco chewer. The nonunion needed special oblique views to clearly document radiographic nonunion (Fig. 2). All patients had neither a coronal/sagittal malalignment of > 15° nor a shortening of > 1 cm.
The mean time for return to the original activities was 64 days (range, 36 to 182 days). The mean time for confirmed radiographic union was 45 days (range, 34 to 180 days).
The mean Constant score was 95.73 ± 5.76 (range, 79 to 100), mean Mayo elbow score was 95.94 ± 6.74 (range, 85 to 100), and mean DASH score was 1.56 ± 3.15 (range, 0.0 to 14.0). The number of patients achieving ideal/perfect Constant, Mayo elbow, DASH scores was 25 (52.1%), 35 (72.9%), and 34 (70.8%), respectively. The distribution of the scores is provided in Table 2.

Table 2
The Distribution of Improvement of Functional Outcome Scores (n = 48)
| Score | Achieved ideal score | Did not achieve ideal score | p-value |
|---|---|---|---|
| Constant | 25 (52.1) | 23 (47.9) | 0.773 |
| Mayo elbow | 35 (72.9) | 13 (27.1) | < 0.001* |
| DASH | 34 (70.8) | 14 (29.2) | 0.004* |
Values are presented as number (%).
Ideal score for Constant and Mayo elbow outcome measures is 100 and for DASH is 0. The proportion of patients who achieved score 100 for Constant score was not significantly high (p > 0.05). The proportion of patients who achieved score 100 for Mayo score was significantly high (p < 0.001). The proportion of patients who achieved score 0 for DASH score was significantly high (p = 0.004).
DASH: Disabilities of the Arm, Shoulder and Hand.
*p-values by one-sample chi-square test. A p < 0.05 was considered to be statistically significant.
![]()
The mean side-to-side difference for abduction, ER, IR, and FE of the shoulder was 4.9°, 4.0°, 3.3°, and 6.4°, respectively. A noteworthy finding of this study was that the difference in ROM between the operated and non-operated sides, albeit the absolute values seemed small, was statistically significant. Though the differences were statistically significant, no clinical significance could be found according to the overall subjective outcomes assessed using our questionnaire. The ROM values are tabulated in Table 3.

Table 3
Comparison of All ROMs between Operated and Non-Operated Sides (n = 48)
![]()
The majority of patients had no variations in postoperative subjective strengths. As shown in Table 4, the proportion of patients who achieved maximum strength for each parameter is significantly higher for the majority.
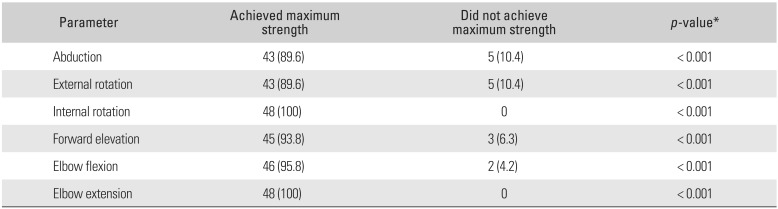
Table 4
Comparison of Parameters of Subjective Strength Analysis (n = 48)
![]()
There were 2 cases (4.17%) of superficial infection, which healed with local care and antibiotics. Two patients (4.17%) had tingling over the forearm, which resolved spontaneously over a period of 6–8 weeks. One patient (2.08%) developed a hypertrophic scar (Fig. 3). There were no cases of deep infection or major neurovascular injury. At the final evaluation, 45 patients (93.7%) returned back to their original jobs. The remaining 3 patients (6.25%) had to modify their original occupations (2 of them were the cases of nonunion) due to pain, lack of strength, and feeling of tightness in the operated limb.

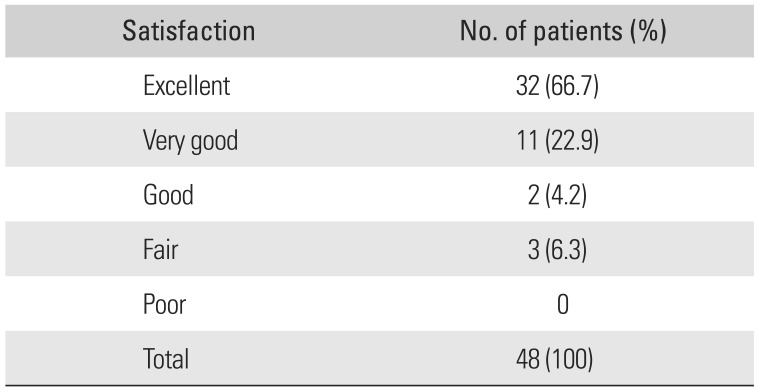
The majority of patients (43 patients, 89.6%) fell in the excellent or very good category of our subjective outcome score. They were extremely satisfied with the results of the procedure and would recommend it to others or undergo the same procedure again, if a need arises. The postoperative subjective outcomes assessed by our questionnaire are presented in Tables 5 and 6.
The mean duration of radiation exposure was 172.5 seconds (range, 111.5 to 247 seconds). The mean surgical time was 95.5 minutes (range, 75 to 132 minutes). Though we did not carry out an exact analysis, the mean values of these variables were inversely proportional to the experience with the technique. The mean blood loss and exact dosage of radiation exposure were not calculated.
Go to :
DISCUSSION
The most important finding of our study is that ABP can be effective in treating mid-shaft humeral fractures in patients predominantly involved in overhead activities with excellent functional and radiological outcomes. The functional outcome achieved in our study is comparable to that in other similar studies on this topic.789101314152122) Compared to the normal opposite side used as a reference, most patients recovered their original ROM and strength. Since there was an apparent discrepancy between the statistical and clinical outcomes regarding ROM (the side-to-side difference was statistically significant but clinically insignificant and it was not possible to account for inherent differences between the dominant & non-dominant limbs), we devised a general questionnaire focusing on the subjective outcomes that were of concern to our patients so as to document the actual clinical outcome and satisfaction rates irrespective of statistical variability. According to the questionnaire, the majority of patients were extremely satisfied with the procedure (43 patients, 89.6%) and would recommend the same procedure to others or undergo it again if a need arises. The follow-up rate of > 80% gives additional authenticity to these findings.
As described by Sarmiento et al.,2) the humerus bone has a wide range of acceptability criteria in its reduction and is highly amenable to conservative management. However, it requires the continuous use of a cast/splint for 6–8 weeks, which is usually cumbersome for the patient. This option is not very suitable for young active individuals (athletes and manual laborers) who need to begin their activities at the earliest. So, these patients are better suited for an early operative intervention.
The primary advantage of ABP is the combination of stability with minimal soft tissue and periosteal disruption.48921) Unlike the posterior plating option, it requires a small incision and adheres to the MIPPO principle, which is biologically and cosmetically preferable. In addition, the rotator cuff is spared preventing any major shoulder pathology later on, which is the case in humeral nailing.23) The ABP follows the principle of relative and elastic stability instead of the absolute rigidity in the open reduction and internal fixation (ORIF) achieved by a posterior approach. In the former, healing takes place by secondary healing and callus formation, which is stronger, whereas in the latter, it is done by primary healing without callus formation.4614) The purpose of using a long plate in ABP is to decrease the stress per unit area as by distributing over a larger surface area.24) So this plate, which is placed on the 'anterior tensile surface,' can withstand a larger amount of rotational and bending stresses than the shorter plate.
There are numerous papers on the functional outcome of ABP for humeral shaft fractures in the general population cohort; however, there is a paucity of literature exclusively dealing with patients predominantly involved in overhead activities. The physical demand placed on the upper limbs of these patients is much greater than that in general population. Hence, this study was undertaken to investigate whether the favorable results of ABP could be replicated in them. Throwing is a complex activity involving both the shoulder and the elbow and obviously needs a well-aligned humerus. It involves multiple phases: windup (phase 1), stride (phase 2), arm cocking (phase 3), arm acceleration (phase 4), arm deceleration (phase 5), and follow-through (phase 6).25) A good throwing action needs an intact shoulder, humerus, and elbow. Any discontinuity/pathology in either of the components will hamper the throwing/overhead activity. Hence, the need for a stable humeral fracture fixation without secondarily disrupting the other two components. Also, strenuous overhead activities in manual laboring need a similar milieu for optimal functioning. The potential for rotator cuff damage during conventional antegrade nailing makes it an unattractive option in this population. The posterior plating involves greater soft tissue striping and larger incisional scars. The ABP is the 'logical middle' in this case.
On the downside, the procedure has a steep learning curve and should not be attempted by inexperienced surgeons without supervision. Although we did not carry out a formal study, the amount of intraoperative fluoroscopy exposure required was greater than posterior plating or intramedullary nailing. Though increased risk of radial nerve injury is one of the issues with ABP, our study had no such an event. As described in multiple cadaveric studies, an important thing is to keep in mind the course of radial nerve near the distal end of the plate, which usually lies a few centimeters distal to the point where the nerve pierces the lateral intermuscular septum.7812181920) Sliding of the plate in a wrong fashion, careless drilling for the distal screws, or over-zealous retraction can lead to potentially catastrophic damage. Two cases of forearm tingling in our series were most probably due to neuropraxia caused by one of the above factors. Similarly, the musculocutaneous nerve that lies below the biceps muscle should be meticulously handled.
Another matter of controversy with ABP is whether to use locking or simple cortical screws. Though there have been no formal studies with this regard, we felt that locking screws might make the construct too stiff increasing the risk of nonunion.2426) We used locking screw only in 2 cases (4.17%) with poor bone quality because we were apprehensive about backing out of simple cortical screws. Comparison between these two types of fixation could be an area of further research.
Our study has certain limitations. Firstly, there was no control group to compare our results with and the follow-up rate was not 100 %, which might have introduced a bias in the study. However, the main aim of our study was to assess the utility of ABP in a selected patient population and not to compare this procedure with any other modes of treatment. Secondly, the malrotation of the humerus after union could not be accurately calculated as no postoperative computed tomography scans were done. So, humeral retroversion angle as described by Boileau et al.27) was not evaluated. However, intraoperative reduction was visually confirmed as per the criteria by Krettek et al.16) and approved by one of the senior trauma surgeons with more than 2 decades of experience during surgery. Besides, there was no case of severe rotational restriction in our patients; implying that any major rotational malalignment was unlikely. Walker et al.1) have already stated that up to 30° of varus angulation, 20° of anterior bowing, and 15° of IR deformity generally do not cause any gross functional impairment. Thirdly, in case of sportsmen, we did not evaluate the actual difference in performance in their respective fields before and after the surgery. Fourthly, the measurements of ROM and strength- both being subjective findings- might have introduced an error. Also, as mentioned earlier, there can be a difference in ROM between the dominant and non-dominant sides, which was not accounted for. Finally, according to Wang et al.,15) MIPPO techniques have an increased risk of secondary shoulder arthritis due to malrotation inadvertently caused during surgery. To know the exact incidence of this, a much longer follow-up would be needed and this could be an area of future study.
In conclusion, ABP for mid-shaft humerus fractures is a safe and effective treatment modality yielding high rates of union, excellent functional recovery, minimal biological disruption, better cosmesis, and superior patient satisfaction. Therefore, we would recommend considering this procedure as one of the treatment options in patients predominantly involved in overhead activities in their daily lives.
Go to :
 XML Download
XML Download