

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Shoulder dislocation is relatively rare, but it is the most common joint to dislocate in the body and is frequently encountered by orthopedists in an emergency setting.1) Shoulder dislocation is more frequent among young age groups who are active in sports and daily activity, but recent changes in lifestyle and increased longevity has seen a significant rise in dislocated joint injuries among the elderly population.2) Unlike younger patients, dislocation in this population is often caused by rather minor injuries since with increasing age the soft tissues surrounding the joint become frail and degenerative. Making the diagnosis is not too complicated when a patient visits with related symptoms during the acute phase, and the joint is reduced in relative ease. However, a missed diagnosis by doctors or negligence by a patient to seek medical treatment after a trauma can lead to the exceptionally rare condition of chronic shoulder dislocation. Although this varies according among the literature, chronic dislocation is defined as a case in which the diagnosis was missed for several days to weeks after initial dislocation.34567) They are usually difficult to reduce in the conventional manner, often requiring a surgical procedure in order to reduce and stabilize the joint, and a delay in making the diagnosis and treating the condition generally leads to significant functional and structural deterioration in the patient. Chronic dislocation is mostly seen in elderly and mentally disabled patients, and missing the diagnosis initially in young age groups is also possible when a person has multiple traumas.147) Many look for medical assistance later in the course due to pain, deformity in appearance and disabling function in the joint. For these patients, the pain does not subside over time, and discomfort is not diminished by physiotherapy.134) However, though it is uncommon among chronic dislocations, there have been a few cases where this ailing condition did not incite persistent pain, creating a further postponement in establishing the diagnosis.45) In the case described in this paper, chronic shoulder dislocation was found in a patient after 1 year, with the affected individual experiencing little pain. This patient had not received medical treatment due to an improvement in symptoms and function shortly after an injury. We are thus making a report about this very rare case of asymptomatic unreduced chronic anterior shoulder dislocation found in an elderly patient along with a review of related literature.
CASE REPORT
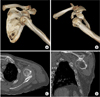
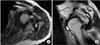
A 72-year-old male patient visited an outpatient clinic due to the deformed appearance of his left shoulder. He suffered fall down injury about a year earlier, and initially the patient had pain and noticed swelling in his shoulder. The patient did not seek medical care immediately after the injury, and because the pain subsided gradually over a week, he did not consult with a physician for 1 year until he presented to Department of Orthopedic Surgery of Wonju Severance Christian Hospital. At the time of the visit, the patient complained of some discomfort from reduced range of motion, but he stated that it did not interfere with his daily activity. Other than a previous cerebrovascular accident and hypertension, his medical history was unremarkable. On physical examination, prominence of the anterolateral border of the acromion and atrophy in the deltoid muscle was observed in the left shoulder (Fig. 1). Passive forward elevation and abduction was within a normal range, but passive external rotation and internal posterior rotation was limited to 25° and to the level of fourth lumbar vertebrae, respectively. Active forward elevation, and abduction and external rotation, were measured to be 130° and 80°, respectively, but active internal posterior rotation and external rotation was severely limited (Fig. 2). On simple radiography, an anteriorly dislocated humeral head was observed, and a Hill-Sachs lesion was also evident (Fig. 3). For further evaluation, three-dimensional computed tomography (CT) was performed. The CT also revealed an anteriorly dislocated humeral head, and the posterior portion of the head with the anterior aspect of the glenoid had formed a false joint. Degenerative change was present within the shoulder joint, and there was a bone defect of about 30% on the glenoid surface (Fig. 4). Magnetic resonance imaging (MRI) was performed to evaluate soft tissue injuries since dislocation is frequently associated with labral and rotator cuff injuries. On MRI, there was a full thickness tear in supraspinatus and infraspinatus tendons. In addition, Hill-Sachs lesions were confirmed (Fig. 5). At the time of initial presentation, the constant score, and the Disabilities of the Arm, Shoulder and Hand (DASH) score, were 75 and 35, respectively. Closed reduction was attempted gently under sedation. However, chronicity of the dislocation made closed reduction impossible, and multiple attempts had failed. The patient received an explanation regarding possible treatment regimes for his condition, both conservative and surgical (reverse total shoulder arthroplasty). Because he did not have any dissatisfaction in performing daily activity, the patient opted for conservative management. He was followed up regularly, and there was no further progression of symptoms or any evidence of newly developed complications at 20 months after his initial visit. The constant and DASH scores measured at the last follow-up were 73 and 37.5, respectively, showing minimal change from the scores measured initially. The patient was informed about the study and provided consent for publication of this article.
DISCUSSION
Managing shoulder dislocation is challenging when the diagnosis is missed or neglected,8) and if the dislocated joint is not reduced immediately after the injury, the chance of repositioning the joint by closed manipulation diminishes considerably over time, while complications associated with closed reduction substantially increase due to fibrotic soft tissues. Chronic shoulder dislocation frequently occurs in elderly patients, especially in those with dementia, and it was found in one study that most patients with chronic shoulder dislocations belonged to age groups between the sixth and ninth decades.3) Although there have been several cases of chronic shoulder dislocation in young patients, these are very rare unless they are hospitalized for multiple traumas and in a comatose mental status in which initial evaluation is both very limited and delayed.4) Young patients with alcoholism or epilepsy are also more likely to come to a clinic with the presentation of chronic dislocation.167) In addition, once the initial pain and swelling subside without significant dysfunction in the joint, patients choose not to seek medical consultation, and even if a patient decides to visit a clinic some time after the injury, the chance of making the diagnosis is further reduced since these symptoms and signs become less evident than immediately after the injury. At first these patients usually have minimal pain and insignificant dysfunction, and these become unnoticed for several months to years until further deterioration of the patient's function and symptoms trigger them to look for medical evaluation and management.1)
Upon reviewing the available literature, it was found that many terminologies and durations are used to describe chronic shoulder dislocation. Although most authors defined delayed diagnosis of shoulder dislocation of more than 3 weeks as chronic shoulder dislocation, other authors stated cutoff points of as early as 24 hours to 1 month for the division between acute and chronic cases.3) Furthermore, there are various nomenclatures used to describe this condition, and these include chronic, unrecognized, missed, old unreduced, chronic unreduced, and ancient dislocations.3) Although they are different, and that these terms may provoke some confusion among orthopedists, they are not too dissimilar to one another. However, one must be careful not to confuse irreducibility with chronicity. To clarify various descriptions of the problem, a study proposed a simple classification.3) It suggested that dislocations of more than 1 week old should be defined as chronic, and that these cases should be further divided into early, late, and ancient groupings. Early chronic dislocation refers to dislocations that are found between 1 and 3 weeks after injury. Any dislocations found between 3 and 12 weeks are termed late chronic, and ancient chronic dislocation includes all dislocations that are older than 12 weeks.
As there is a conflict about defining what chronic shoulder dislocation is, the strategy for how to manage the problem is also controversial and remains a challenge.4) Currently, there is not an established treatment protocol, and the management methods performed by authors in previous studies are experimental or based more on experiences rather than based on evidence. There are sporadic publications that explain various methods for treating chronic dislocation. These methods include no treatment, closed manipulation, open reduction with or without fixation and resection arthroplasty, and recent additions of arthroscopic reduction with repair of associated labral and rotator cuff injuries, and joint replacement.13578) Although reduction is relatively easy in most cases of acute shoulder dislocation, it will become nearly impossible in chronic cases to reduce a joint that has been dislocated for more than 2 weeks. One study suggested that attempts to reduce the joint should be dropped if the dislocation has been left for more than 6 weeks.3) The reasons for the limited chance for closed manipulation are soft tissue interposition and fibrosis, bony obstacles, or a combination of both.79) In addition to its high failure rate, closed reduction should be performed in a gentle manner since an overly forceful maneuver can lead to complications such as fracture and traction injury of the neurovascular structures around the joint. Sudden and aggressive efforts may result in traction or an even worse transecting injury to these tissues.9) For elderly individuals with a chronic shoulder dislocation, the risk for complications related with closed manipulation is even higher.8)
If an attempt on closed manipulation fails or is not considered a viable option, open reduction is the next step.4) Because extensive fibrosis is present in the shoulder joint that has been dislocated for a long time, a meticulous release of capsule and other soft tissues is necessary to reduce the joint without tension; otherwise abnormal soft tissue tension may have an adverse effect in maintaining the stability of the joint. In addition, the glenoid surface itself is obliterated with scar tissue and loose bodies and must be cleared prior to reduction.1) If the reduced humeral head is stable, fixation is not required necessarily, and stability can be preserved by positioning the arm in a sling at the side anterior and posterior to the coronal plane of the body for anterior and posterior dislocations, respectively.16) However, chronicity of the dislocation generally demands some form of fixation in the early postoperative phase due to the high risk of redislocation. This is a temporary application to prevent redislocation until the soft tissues heal. Although it has been reported to be effective,568) the method causes injury to the articular surfaces of the humeral head and glenoid. In addition, fixating the articulation may prevent the possible beneficial effects of early shoulder motion, which improves articular cartilage nutrition.16)
In recent years, advancements in surgical techniques and equipment has led to less invasiveness, more options and better outcome in treating chronic shoulder dislocations. Upon reviewing the available related articles, it was found that the latest articles lean more toward arthroscopic management for early chronic shoulder dislocations, and joint arthroplasty for the more prolonged dislocations with significant structural deterioration. Arthroscopic reduction can be performed before soft tissue contractures do not become permanently rigid.7) Indications suggested by one study comprise of intact and healthy articular cartilage, humeral head defect of less than 20%, and presence of a loose body in the glenohumeral joint space.110) Shoulder dislocation is often associated with rotator cuff tears, Hill-Sachs or Bankart lesions, labral avulsion or superior labral tear anterior to posterior injuries.2) The advantage of arthroscopic management is that it allows direct access to and inspection of these intra-articular problems within the joint. In addition, repair of labroligamentous structures through arthroscopy can give the initial stability needed to prevent postoperative subluxation or redislocation,67) and thus it has the potential benefit of better functional outcome by allowing the possibility of early postoperative rehabilitation.
On the contrary, arthroplasty is recommended for patients with severe structural deterioration of bone and cartilage.578) Prior to progression in shoulder arthroplasty techniques and implants, resection arthroplasty and arthrodesis had been alternative treatment methods for such patients with extreme defects, but while pain is eliminated, function of the joint is completely lost after these procedures.8) Thus, by replacing the joint, a patient has an opportunity to recover some function of the affected joint. One study has suggested indications of arthroplasty that include damaged and unviable joint surfaces, a humeral head defect of more than 40% of the articular surface, and a dislocated state of more than 6 months.1) If the dislocation has existed for more than 6 to 12 months and the humeral head has not been in contact with the glenoid surface, subchondral bone becomes osteopenic and soft.4) There is then as considerable risk of head collapse and flattening after reduction.1) The same study that suggested the indications for arthroplasty reported satisfactory outcomes in 9 of their 10 patients.
Whether it is chronic or not, the goals for treating shoulder dislocation is prevention of further redislocation and recovery of an acceptable range of motion and strength of the extremity, in order to at least maintain daily activity.2) For most of the patients with shoulder dislocations, pain and functional deficit are sufficiently significant as to interfere with the activities of daily living. Although there have been several reports of chronic shoulder dislocations with remarkably minimal pain and reasonably good range of motion, over time functional deficits and symptoms will eventually develop, potentially to the point of becoming unbearable to the patient.1348) Conservative management options such as physiotherapy are not effective or may cause further damage to the joint. Thus, an earlier operation provides a better outcome, although it was found that functional recovery was not related to the duration of dislocation.3) In our case, after failure in attempts for closed reduction, we recommended the patient undergo reverse total shoulder arthroplasty because the dislocation was nearly a year old, and there was evidence of arthritic change and rotator cuff injury from imaging studies. However, to our surprise given our initial negative view on the patient's progress, follow-up at 20 months revealed that he had been free of disabling pain and had maintained satisfactory function with negligible decline from the values measured at the initial visit.
Above all, the best treatment option for chronic shoulder dislocation is to prevent the acute dislocation from progressing into the chronic condition in the first place by making a prompt and accurate diagnosis. It is imperative to pay more attention to patients who are at risk of missing the diagnosis, and thorough examination should be performed when suspicion is high. Appropriate diagnostic tools for observation of the axillary lateral view in addition to standard simple radiographic series10) are essential to confirming the diagnosis, and if necessary CT can be considered in assisting a more accurate evaluation of the chronic dislocation. Once chronic shoulder dislocation is diagnosed, closed reduction of the dislocation can be attempted. Although reducing the dislocation is considerably difficult and unsuccessful in most cases, it is still recommended that reduction be performed since it still has some positive effect on function. When it fails, open surgery is recommended, but, when choosing an operative mean, the presence of comorbidities, the patient's functional demand prior to the injury and their expectations, must also be taken into account.278) To these patients, excessive and unnecessary treatment, whether it is a closed or open technique, may cause harms that outweigh the benefits. There are very few cases of individuals with a chronically dislocated shoulder remaining asymptomatic and maintaining reasonable function despite having no proper manipulative treatment; but clinicians should be reminded that no action can be the best possible treatment in a certain number of patients.



 XML Download
XML Download