

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Developmental coxa vara is a hip deformity characterized by a defect in endochondral ossification of the medial portion of the femoral neck, together with the progressive vertical inclination of the proximal femoral physeal plate and shortening and decrease of neck shaft angle.1) The natural history of coxa vara may be debilitating as the child develops progressive limb length discrepancy, limp pain, abductor weakness, and restricted motion. Secondary acetabular dysplasia and genu valgum may compound the problem. With the exception of some forms of developmental coxa vara that can resolve itself, a variety of surgical methods have been developed to deal with progressive coxa vara.2) There is a general agreement in the literature that a valgus osteotomy at a trochanteric or subtrochanteric level is the most definitive method for achieving the surgical correction, which means the correction of the neck shaft angle and horizontal reorientation of the growth plate. Nevertheless, there is no consensus in the literature regarding the details of osteotomy and fixation method.1234) The purpose of the present study was to evaluate the short-term results of the intertrochanteric valgus Y osteotomy with internal fixation using a contoured T plate.
METHODS
Informed consent was obtained from all parents of the individual participants included in the present study. This prospective study was conducted from January 2010 to December 2013 at Zagazig University Hospitals. Eighteen corrective intertrochanteric valgus Y femoral osteotomies were performed in 18 patients (18 hips) for treatment of unilateral developmental coxa vara deformity fixed with a T-buttress plate for stabilization. The main indications of intertrochanteric valgus Y femoral osteotomies were the presence of shortening and the inferomedial triangular fragment of the neck that was not clear in all cases. They were 12 males and 6 females. The right hip was affected in 10 patients and the left hip in 8 patients. The average age at first presentation was 6.1 years (range, 5 to 7 years). All the patients included in the study had developmental coxa vara. Any patients with coxa vara of other etiologies, congenital, dysplastic, or acquired as infection or trauma were excluded from the study. The patient's chief complaints were limping with minimal or no pain. The signs that were revealed by physical examinations in all patients were short leg gait with an abductor lurch, positive Trendelenburg test, and limitation of abduction and internal rotation of the involved hip. The patients were evaluated clinically by Larson score (Iowa hip score).5) Anteroposterior (AP) view of the pelvis was obtained to measure the Hilgenreiner-epiphyseal angle (HEA) and the femoral neck-shaft angle (FNSA) and the frog leg lateral view for the assessment of the femoral anteversion was taken preoperatively, then monthly until 1-year postoperatively, and at the final follow-up. Limb scanograms for measurement of limb length discrepancy were done preoperatively and at the last follow-up in all patients.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Statistical Analysis
Statistical analysis was performed using SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). Wilcoxon signed-rank test was used for statistical analysis of the results and p < 0.05 was considered statistically significant.
Preoperative Planning and Operative Technique
The angle of correction was determined by tracing paper on the plain AP radiographs of the pelvis taken with both hips in neutral rotation. The surgery was performed using the straight lateral approach to the proximal femur. The T-shaped plate (Synthesis plate and screw; Tantawi Medical Co., Cairo, Egypt) was contoured to the desired angle of correction. After removal of a triangular wedge, the osteotomy was closed. The most proximal screw was tightened and the second screw in the femoral neck was inserted. The distal fragment was secured to the plate by at least four screws starting by the proximal oblique screw in the oval hole just below the planned osteotomy site to allow compression at the osteotomy site. Wound was closed in a usual manner and drain was removed 48 hours after surgery. Postoperative immobilization in a hip spica cast was performed for 6 weeks. Full weight bearing was delayed up to 2 months after surgery.
RESULTS
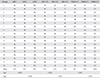
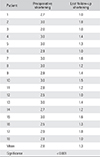
The average follow-up was 29 months (range, 24 to 36 months). The clinical results showed improvement of the mean Larson (Iowa) hip score from 57.8 to 97.0 (p < 0.001) at the last follow-up. The radiological results showed that all the osteotomies were completely united in 2.4 months (range, 2 to 3 months), with the achievement of the planned correction angle. The average correction of the HEA was improved from 78.2° to 27.8° (p < 0.001) at the last follow-up. The FNSA was improved from 93.7° to 129.9° (p < 0.001) at the last follow-up. The shortening of the affected limb was corrected from 2.8 cm to 1.3 cm (p < 0.001) at the last follow-up measured using scanograms. Avascular necrosis, hip subluxation, premature proximal femoral physeal closure, or any serious complications were not encountered. Three patients developed keloid formation of the surgical scar. At the last follow-up, no significant or minimal recurrence of deformity was reported (Tables 1 and 2, Figs. 1, 2, 3).
DISCUSSION
There are limited choices of implants that allow secure fixation of the underlying proximal femoral osteotomy, and the selection can be particularly small in young children. Furthermore, any fixation device needs to avoid the proximal femoral growth plate, leaving a limited length of bone available for secure fixation.134) Even in cases of well-performed osteotomies, the literature cites recurrence rates of 30%–70%.6) When the HEA was corrected to < 38°, 95% of children had no recurrence of varus deformity. Some authors also recommended an overcorrection of the HEA to the normal (anatomic) value of 22° to ensure no recurrences.7) In contrast, the head-shaft angle was not found to be a reliable indicator of appropriate correction. The recurrence was mainly due to the loss of correction angle resulting from a weak fixation. Carroll et al.7) found no strong correlation between the postoperative neck shaft angle and lasting good clinical outcomes. They reported that the most consistent and reliable predictor of outcome was the HEA. Typically, an ideal implant should be rigidly applied to the underlying bone, making appropriate lateral translation of the distal fragment to avoid medial displacement of the osteotomy, which would exacerbate loading of the lateral compartment and distal femoral physis.8) Depending on the postoperative stability, some of these children may need a hip spica cast for several weeks after surgery to prevent any displacement at the osteotomy site.9) The objective of this study was to evaluate the application of a contoured T plate for fixation of intertrochanteric valgus Y osteotomy in treatment of developmental coxa vara; therefore, the focus was set on this specific implant and its handling. The T plate was designed by the Arbeitsgemeinschaft für Osteosynthesefragen (AO) group to meet the anatomic biomechanical requirement mainly in the metaphyseal areas of the bone.10) It was designed to buttress a thin cortex, to prevent a defect in cancellous bone from collapsing, or to be occasionally used as a tension band plate so as to simply prevent axial deformity resulting from shear or bending. Thus, it must be applied to the cortex that has been broken, osteomatized, or under load. In spite of being relatively thin, this plate can be found sufficiently strong if used for proper indications.
The T plate has an oval hole. This hole permits some up and down adjustments and also an oblique lag screw to be inserted through to bring the osteotomy under interfragmentary compression, enabling the plate to be used as a tension band plate.10)
The treatment of choice for developmental coxa vara has followed the recommendations of early work by Amstutz, Freiberger and Wilson in the use of either subtrochanteric or intertrochanteric osteotomies.23) Both methods have their own merits and defects.123468111213) Regarding the intertrochanteric osteotomies, the Pauwels' Y-shaped and Langenskiold valgus-producing osteotomies have been shown to provide good results. However, these osteotomies have a somewhat limited ability to correct the associated femoral neck retroversion.1415)
The subtrochanteric valgus-producing osteotomies used by many authors also have provided good and lasting clinical results. The great advantages of the intertrochanteric osteotomy over the subtrochanteric osteotomy include that it is done in the metaphyseal highly cancellous proximal femoral bone with high power of union, which is nearer to the site of the hip deformity with easier deformity correction and also it obviates radiologic disadvantage of a subtrochanteric osteotomy, which is the creation of a secondary angular deformity in the form of femoral shaft kinking distal to the primary deformity.78141617) On the other hand the authors reported that this radiological kinking remodels significantly and has no negative influence on hip function.4) In the present study, the length of the oblique limb of the Y-shaped osteotomy was fixed to be one-half of the diameter of the femur at the level of the osteotomy. This modification was taken from the original Pauwels' osteotomy where the length of the oblique limb of the Y-shaped osteotomy is determined based on the inferomedial triangular fragment of the neck which is not clear in all cases. In addition, the procedure requires smaller bone resection at the base of the wedge on the lateral cortex, consequently resulting in less postoperative shortening.8) In the present study, the average correction of HEA was significant, with insignificant or minimal recurrence of the deformity in all cases and significant improvement at the last follow-up of the mean Larson (Iowa) hip score. This was also evident in the biomechanical works of Pauwels11) and Carroll et al.7): the correction of the HEA to less than or equal to 45° with secure postoperative fixation is a crucial factor for prevention of deformity recurrence or loss of correction. In this study, we also faced some limitations that had been faced by other authors in the literature: the small study population and the lack of long-term fellow-up. In summary, the type of osteotomy may be less important than achievement of surgical correction, especially correction of the neck shaft angle to a more physiologic angle and HEA to less than 35°–40°, correction of femoral anteversion (or retroversion) to more normal values, ossification and healing of the defective inferomedial femoral neck fragment, and reconstitution of the abductor mechanism through the replacement of its normal length-tension relationship.718) Furthermore, there are successful reports on a new locking compression pediatric hip plate, which allows corrective osteotomies of the proximal femur and surgical treatment of femoral neck fractures in a safe way and provides the possibility of weight bearing based on biomechanical properties of locking screws.19)
In conclusion, the use of T plate for fixation of trochanteric valgus osteotomy in the treatment of the developmental coxa vara appears to be a reliable treatment and good solution for stable fixation of the osteotomy without nonunion, loss of correction, or deformity recurrence.



 XML Download
XML Download