

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Morphometric analysis of anatomy can be very valuable to a surgeon when assessing patient-specific implant needs prior to commencing any orthopedic procedure.1234) An analysis may occur on the micro-scale, where the surgeon evaluates an independent patient for surgical planning, or on the macro-scale, wherein populations as a whole are analyzed for trends or relationships. Values generated from the latter type of analysis could be valuable for improving the design of implant systems to better suit the needs of specific patient populations. While there are a number of arthroplasty systems available on the market that offer multiple implant sizes, these devices were designed with the population of the USA and Western Europe in mind.567) Increases in international trade, such as between North America and East Asia,8) may raise the concern that utilizing existing systems tailored for the Western world would be suboptimal in an East Asian population. Previous work from Aroonjarattham et al.9) directly compared datasets of a Thai population and a USA cohort: their findings indicated that the former group displayed, on average, a smaller humeral head. Other studies of a similar scope have also reported that the USA populations exhibit larger humeral head measurements overall.3410) In addition to these morphometric findings, anthropomorphic data from large scale studies indicate that the East Asian population is smaller overall in terms of both height and weight.111213) While it could be inferred that there would likely be sizing issues due to the differences associated with height and, therefore, shoulder size,14) there may also be other morphologic differences within the shoulder joint that have not been described. While these morphologic differences are likely small, their potential impact on shoulder kinematics and resulting clinical outcomes merits in-depth analyses of these populations. Using a set of prescribed metrics of the anatomic and glenohumeral relationships of the shoulder,14) the purpose of this study was to determine the morphologic and spatial differences, if any, between North American and East Asian populations.
METHODS
This study was approved by the Western Institutional Review Board (Olympia, WA, USA). Morphologic data from 92 North American patients were derived from our prior study.14) The patient-reported ethnicities of this group included Caucasian (90%), Native American (4%), African American (4%), and Hispanic (2%). There were no patients with a self-reported Asian background in this cohort. These patients were from a single institution of the senior author, had a preoperative diagnosis of severe rotator cuff deficiency, and received computed tomography (CT) scans with 1.25-mm slice thickness (GE Lightspeed Qz/I helical scanner; GE Healthcare, Waukesha, WI, USA) in the supine position. A convenience sample of 58 East Asian patients who underwent open reduction internal fixation (ORIF) for a clavicle fracture with preoperative CT scans of the shoulder (Philips Brilliance 64 CT Scanner; Philips Medical Systems, Cleveland, OH, USA) was analyzed as a comparative demographic cohort. Demographic data (height, weight, and gender) were acquired for all patients in the North American and East Asian cohorts. Study patients displayed little to no glenohumeral wear, osteophytes, or osseous defects as determined by a fellowship-trained orthopedic surgeon. The CT scans were imported into Mimics 14.12 (Materialise, Leuven, Belgium) and three-dimensional (3D) renderings of the proximal humerus and scapula were generated. Models were then imported into SolidWorks (Dassault Systemes, Véilzy-Villacoublay, France) as computerized assisted drawing entities.
Definition of Landmarks and Coordinate Systems
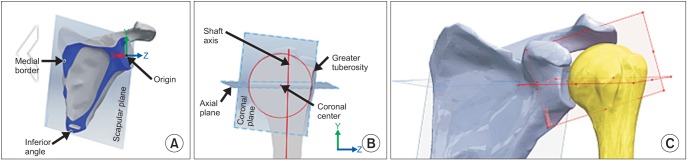
The analysis methods used were identical to our prior methodology (Fig. 1).14) A set of prescribed points denoting specific anatomic landmarks of the scapula and humerus were marked (Fig. 2 and Table 1) and used to develop scapular- and humeral-based coordinate systems to assist with measurement of shoulder joint metrics. The scapular plane (Fig. 1A) was defined by 3 intersecting points along the medial border, inferior angle of the scapula, and glenoid center (Fig. 2D; point F). For the humerus (Figs. 1B and 2A), the humeral coronal plane was defined using the humeral shaft axis and a point on the greater tuberosity (H). The shaft axis was created using the centers of 2 best-fit ellipses corresponding to 2 unique axial cross-sections of the humeral shaft in the 3D model. The greater tuberosity was identified as its most lateral point opposite to the humeral head's surface center. Points were marked along the cross-sectional coronal plane to denote the borders of the humeral head's articular border and neck shaft. A best-fit circle was placed along the articular border to determine humeral head center (G) and radius of curvature (G, L). The angle from the articular margins of the head from the head center was used to measure the articular angle (β). These articular margins were also used to define the line of the humeral neck and the neck shaft angle (α). In turn, the neck shaft line's center was utilized to define humeral head thickness (J, K). The humeral head center was used to supply the location for the orthogonal axial plane, and similarly the articular border of the humeral head was used to define a best-fit circle for the axial plane head radius of curvature (N, O). The most lateral point of the acromion was marked (I) along with points corresponding to borders of the glenoid height (P, Q), and the superior (R, S) and inferior glenoid width (T, U). Coordinates of all glenoid points were recorded to quantify the magnitude of each metric.
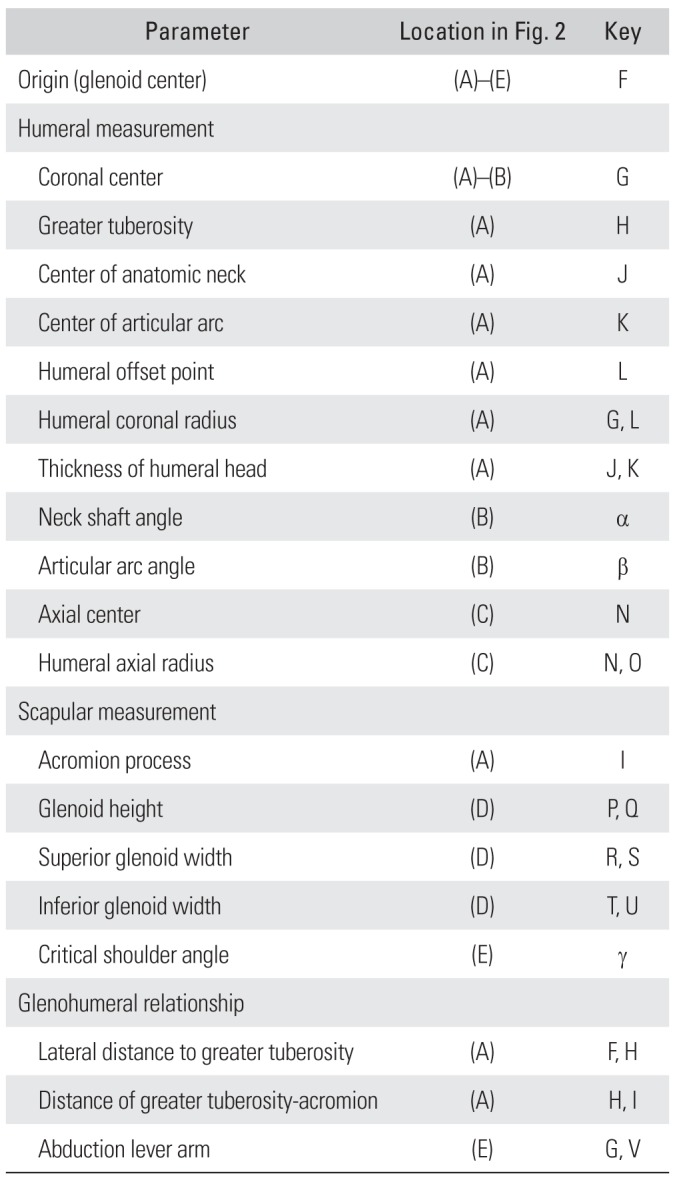
 | Fig. 1(A) Scapular plane derived from the anatomic landmark points and derived coordinate system. (B) Humerus coronal plane as determined from greater tuberosity and shaft axis, with perpendicular axial plane from coronal head center. (C) Alignment of scapular and humeral planes, creating a nonpathologic positioning of the humerus.
|
 | Fig. 2Diagram of measurements taken from each patient in the humerus (A–C), scapula (A, D, E), and glenohumeral joint (A, E). Key available on Table 1.
|
Table 1
Anatomic and Relationship Metrics Key Used in Fig. 2
| Parameter | Location in Fig. 2 | Key |
|---|---|---|
| Origin (glenoid center) | (A)–(E) | F |
| Humeral measurement | ||
| Coronal center | (A)–(B) | G |
| Greater tuberosity | (A) | H |
| Center of anatomic neck | (A) | J |
| Center of articular arc | (A) | K |
| Humeral offset point | (A) | L |
| Humeral coronal radius | (A) | G, L |
| Thickness of humeral head | (A) | J, K |
| Neck shaft angle | (B) | α |
| Articular arc angle | (B) | β |
| Axial center | (C) | N |
| Humeral axial radius | (C) | N, O |
| Scapular measurement | ||
| Acromion process | (A) | I |
| Glenoid height | (D) | P, Q |
| Superior glenoid width | (D) | R, S |
| Inferior glenoid width | (D) | T, U |
| Critical shoulder angle | (E) | γ |
| Glenohumeral relationship | ||
| Lateral distance to greater tuberosity | (A) | F, H |
| Distance of greater tuberosity-acromion | (A) | H, I |
| Abduction lever arm | (E) | G, V |
![]()
Quantification of Glenohumeral Relationships
Humeral and scapular planes were used to reposition the humerus from its initial state to an ideal nonpathologic orientation (Fig. 1C). A soft tissue lateral offset of 4 mm between the glenoid and humeral head was used to standardize the thickness of articular cartilage in all patients (F, L).15) Both of these adjustments allowed statistical comparison to our prior work14) and use of our published glenoid height classification, which defines small, medium and large glenoid heights as < 33.4 mm, 33.4–38.0 mm, and > 38.0 mm, respectively.14) The coordinates for the adjusted humeral points were recorded and relative distances in each axes from the scapular landmarks were determined. The lateral distances to the greater tuberosity and acromial margin were measured. These measurements quantified the acromial index (AI), repurposing the methods used for plain radiographic measurements into our 3D model.16) For our purposes, the ratio of the distances of the lateral acromial (F, I) and greater tuberosity (F, H) were used relative to the scapular coordinate system. In addition, the critical shoulder angle metric utilized by Moor et al.17) was also implemented in a modified fashion relative to the scapular coordinate system used in this study (γ). The abduction lever arm of the middle deltoid (G, V) was determined according to a modified methodology of Cabezas et al.14) and Lemieux et al.18)
Statistical Analysis
Measurements derived from both populations were evaluated for normality using Shapiro-Wilk test. Normally distributed data were compared between populations using an independent t-test (IBM SPSS ver. 20; IBM Co., Armonk, NY, USA) while a nonparametric Mann-Whitney U test was used to compare data that failed the normality test. Statistical significance was set at p = 0.05.
Go to : 
RESULTS
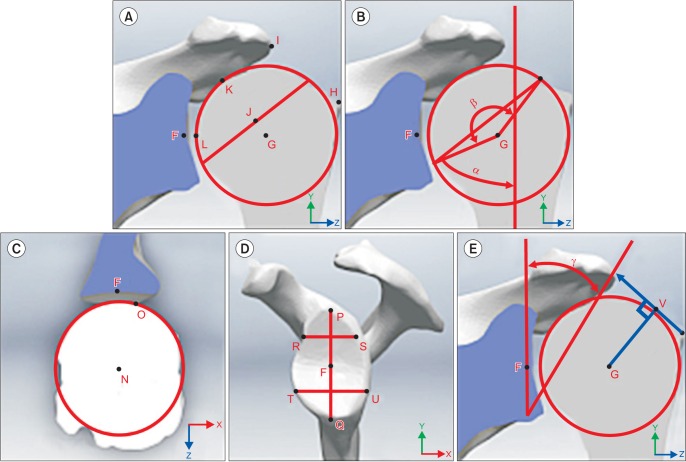
The North American patient population was comprised of 48 females and 44 males (average age, 71 years.) while the East Asian population was comprised of 35 males and 23 females (average age, 69 years). Comparative data are presented in Table 2. The East Asian cohort was shorter (p = 0.038) and weighed less (p < 0.001). The smaller size of the East Asian population was also indicative of smaller values for each shoulder-related metric when compared to the North American group, with a few exceptions. In the East Asian group, the length of the acromion from the glenoid was greater compared to the North American group by an average of 3.6 mm (p < 0.001), which translated into a larger mean critical shoulder angle (p < 0.001). The abduction lever arm was not different between groups (p = 0.408), nor were the neck shaft and articular arc angles (p = 0.305 and p = 0.185, respectively). The AI was significantly larger in the East Asian group (p < 0.001). Applying our previously published classification schema for glenoid height to the East Asian group, 50% were small, 46.8% were medium, and 3.2% were large. When analyzing gender differences between groups, the male subjects were found to exhibit all of the same statistical conclusions (Table 3). As with the entire population, most of the metrics were smaller for the male East Asian group compared to the male North Americans, with the exception of the acromion length, which was again larger for the male East Asian group (average difference = 2.8 mm, p = 0.003). Consequently, the AI was also found to be larger for the male East Asian group (p < 0.001). The angles were found to be no different between groups, as was the abduction lever arm measurement (p = 0.061). The female subjects were also found to have similar findings (Table 4), with a difference in mean acromial length of 3.8 mm (p = 0.001). The AI was larger for the female East Asian group compared to their female North American counterpart (p < 0.001).
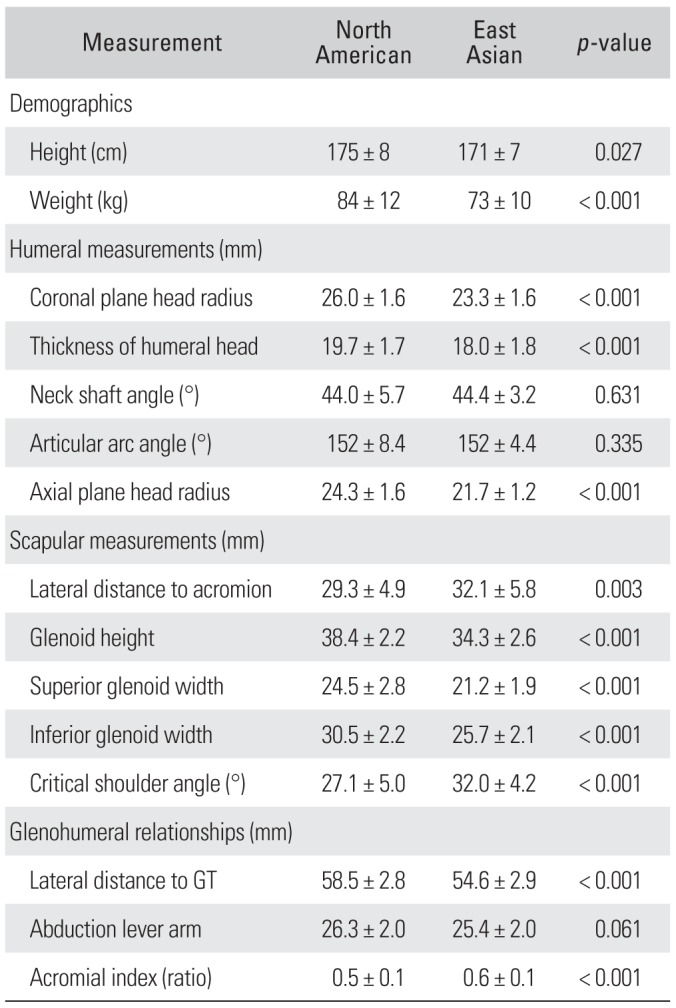
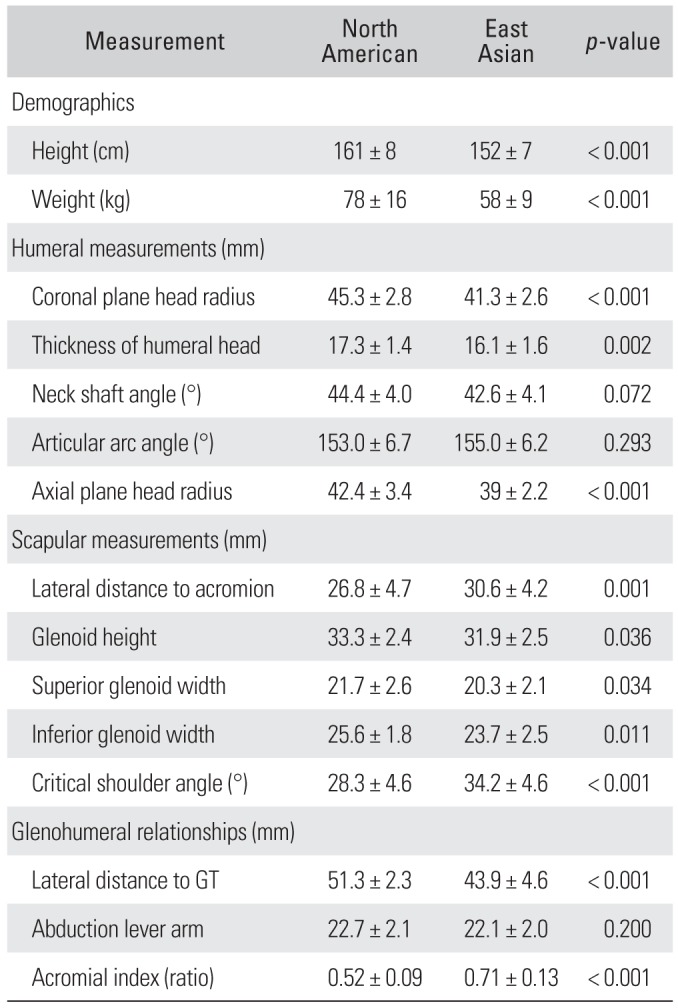
Table 2
Metrics for North American and East Asian Groups
![]()
Table 3
Metrics for Males of Each Group
![]()
Table 4
Metrics for Females of Each Group
![]()
Go to :
DISCUSSION
The majority of results in this study were unsurprising, given that the anthropomorphic metrics of height and weight were smaller in the East Asian group. However, we did identify small morphologic differences between the two populations, which may impact (1) how we view and analyze shoulder anatomy and (2) how we understand the development of specific shoulder pathologies. It also provides insight regarding surgical procedures performed around the shoulder girdle, particularly relating to the area of shoulder arthroplasty.
Study results indicate significantly smaller metrics in nearly all measurement categories in East Asians compared to North Americans. On average, coronal and axial plane head radii were approximately 2 mm smaller in East Asians. While the clinical meaning of this difference is unknown, it may be used as a design consideration by manufacturers of shoulder arthroplasty humeral head components intended for use in patients of East Asian descent. Currently, most arthroplasty prosthesis systems are based on average sizes for USA and European populations.567) In the setting of glenohumeral arthritis, placing a small humeral head component into a small East Asian patient may lead to overstuffing of the joint, as the implanted head does not translate to a small component for this population. Such a scenario may lead to stiffness, pain, component loosening, and a potentially inferior outcome. Perhaps the most unexpected finding of this study was that the East Asian group displayed a larger lateral acromial offset and AI while maintaining an equivalent abduction lever arm to their North American counterparts. Several studies have explored the potential correlations between scapular morphology and different types of shoulder pathologies. Nyffeler et al.16) were the first to examine the relationships between AI and the potential for developing rotator cuff tears (RCTs) and glenohumeral osteoarthritis (OA). They compared the AI in the following three age- and gender-matched groups: (1) a full-thickness RCT group; (2) a glenohumeral OA with intact rotator cuff group; and (3) a volunteer control group with intact rotator cuff. The RCT group demonstrated a mean AI of 0.73, while the AI for the OA with intact rotator cuff group was 0.60. Their findings showed that a longer lateral extension of the acromion correlated with the development of rotator cuff pathology, whereas a shorter extension likely confers some protective effect.
In a comparison morphometric study, Yu et al.19) found a positive correlation between an increase in AI and subacromial impingement when compared to a normal control group. They also showed that patients with a lower AI demonstrated higher rates of traumatic instability. These findings were corroborated in another morphologic study by Torrens et al,20) in which they compared the AI between a cohort of patients with rotator cuff tears and a control group without rotator cuff pathology. They again showed that the group with rotator cuff pathology had a significantly increased AI compared to the normal controls. The initial findings of Nyffeler et al.16) have been substantiated in a recent follow-up case-control study by Moor et al,17) wherein patients with rotator cuff tears demonstrated significantly higher AIs. They also found that the critical shoulder angle, which is a measure of acromial length and glenoid inclination, was the best predictor for developing an RCT.
Despite an apparent correlation between AI and rotator cuff pathology, conflicting findings have been seen in other studies. Miyazaki et al.21) have performed the only study, to our knowledge, to specifically analyze the association of AI and rotator cuff pathology between two distinctly different nationalities. They found a significant correlation between an increased AI and greater rates of RCTs in a mixed Brazilian cohort, but no association in a homogenous Japanese population. Similarly, in a prospective cross-sectional study by Hamid et al,22) they found no association between AI and full-thickness RCTs. There was a significant association, however, between the presence of an acromial spur along the insertion of the coracoacromial ligament and a full-thickness RCT.
This study had several limitations. It utilized the dataset generated from our prior work and, therefore, the results from the original population were not independently validated or re-measured. However, the interobserver measurement reliability was high (intraclass correlation coefficient, 0.794) in our original investigation.14) Given the smaller anthropometric and measured morphometric features of the East Asian cohort reported herein, it may be reasonably assumed that reproducibility of the measurement technique in this population using identical methods as in our prior work would be high as well. Secondly, the two data sets presented here represent patients treated by single surgeons in both patient cohorts. Consequently, there may be a higher degree of variability in each population than reported in the current work. However, large-scale anthropomorphic studies indicate that our height/weight means for each group are well within a standard deviation of previously reported metrics.111213) Thirdly, the number of East Asian female subjects was smaller than the number of male subjects and this may have skewed the morphometric measures to be higher. However, to account for this discrepancy, we performed separate analyses for male and female subjects. Finally, our measurements were made in a pathologic population with artificially positioned humeri, and as such, there may be other morphologic variables that were not considered in this study that would not be observed in normal, healthy controls.
In conclusion, the East Asian population exhibited smaller shoulder morphometrics than their North American cohort, with the exception of an extended acromial overhang. The morphologic data can provide some additional factors to consider when choosing an optimal shoulder implant for the East Asian population, in addition to future designs that may better accommodate this population.
Go to :
 XML Download
XML Download