

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Osteoporosis is a skeletal disorder characterized by bone fragility and increased risk of fracture.12) Life time risk of osteoporotic fracture has been estimated at 40%.1) In addition, the risk of additional fracture following osteoporotic fracture increases from 1.5 to 9 fold.3) The most common site of osteoporotic fracture is spine, followed by hip, forearm, and proximal humerus.4) Among them, incidence of proximal humeral fracture has increased by 3 fold over 30 years.567) The risk of fracture begins to increase linearly as the population ages,4) and history of previous fracture at any site is regarded as an important risk factor for subsequent fractures.8) Especially, humeral fracture can be considered the important prognostic factor for the additional hip fracture, as the incidence of femoral fracture increased 6 fold within 1 year after humeral fracture.9)
Appropriate treatment of osteoporosis is reported to reduce the fracture risk from 40% to 60%, however treatment of the osteoporosis, especially treatment of nonvertebral osteoporotic fracture is poorly practiced.1011) Furthermore, there are few reports for the evaluation and treatment of the osteoporosis after the proximal humeral fracture.
The first purpose of the current study was to evaluate the adequacy of the diagnosis and treatment of the osteoporosis after proximal humeral fracture, and the second purpose was to estimate the pattern of practice for the osteoporosis after osteoporotic fracture.
METHODS
We performed a retrospective nation-wide cohort study. The data was extracted from the nation-wide claims database of the Health Insurance Review Assessment Service (HIRA) of South Korea in 2010, which includes 97% of the Korean populations. All medical facilities submit data for medical records including patient's age, sex, diagnoses based on International Classification of Disease, 10th revision of code (ICD-10), procedure, prescriptions, disposition, medical costs to the HIRA whose database has been used previously for several epidemiologic studies. Fractures were identified by the use of ICD-10 to evaluate the incidence of fractures. Patient aged ≥ 50 years with hip fractures (S720-722), spine fractures (S220, S320, S327-328), or proximal humeral fracture (S422) were included in the present study. Multiple fractures were excluded from the study for the possibility of high-energy trauma. We included only one record to prevent duplication of patients with more than single record in the HIRA. Evaluation and treatment of the osteoporosis after fracture were also analyzed with using the code. The frequencies of diagnostic bone density scan after fracture including the dual energy X-ray absorptiometry, quantitative computed tomography, or ultrasonography were analyzed by the data from HIRA. Furthermore, the prescription rate of osteoporosis medication after diagnoses of osteoporotic fracture was also analyzed. Osteoporosis medication comprised bisphosphonate, selective estrogen receptor modulator, calcitonin, parathyroid hormone, estrogen replacement, and/or vitamin D. Furthermore, authors analyzed the rate of concurrent diagnostic bone density scan and osteoporosis medication after osteoporotic fracture.
Statistical Analysis
All statistical analyses were performed with SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA), and a p-value of less than 0.05 was considered as the level of statistical significance. Chi-square test was used to evaluate the difference in the incidence, diagnosis, and treatment for osteoporosis between fractures. Poisson regression analysis was performed to calculate incidence-rate ratios (IRRs) to compare rates among fractures and the 95% confidence interval (CI) was also estimated.
RESULTS
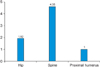
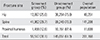
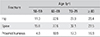
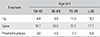
A search of database identified 48,351 hip fractures, 141,208 spine fractures, and 11,609 proximal humeral fractures in patients ≥ 50 years of age in 2010. The incidence rate of fracture including hip, spine, and proximal humerus significantly increased with age (Fig. 1), and those aged ≥ 80 years were the highest. The incidences of fracture were significantly more common in female (2,970/100,000 in women) than male (963/100,000 in men). Among these patients, 12,097 (25.0%) of hip fractures, 41,962 (29.7%) of spine fractures, and 1,458 (12.6%) of proximal humeral fractures underwent diagnostic bone density scans, and the proportion of screened group with proximal humeral fracture was lowest among fractures (p < 0.001) (Table 1). Using Poisson regression analysis, IRR of screened group with hip fractures, vertebral fracture, and proximal humeral fracture were 1.81 (95% CI, 1.71 to 1.91), 2.16 (95% CI, 2.05 to 2.28), and 1.00 (95% CI, 1.00) with adjustment of both age and gender, respectively. Age adjusted and gender specific IRR of screened group were 0.68 (95% CI, 0.66 to 0.69) for male and 1.00 for female. Gender adjusted and age specific rate of screened group were highest in patient aged 70 to 79 years (Table 2). However, the rate of treated group with osteoporosis medication was lower than that of screened group (Fig. 2). Osteoporotic medication rates were 4,773 patients (9.9%) of hip fractures, 27,261 (19.3%) of spine fractures, and 639 (5.5%) of proximal humeral fracture. IRR of treated group with hip fractures, vertebral fracture and proximal humeral fracture were 1.75 (95% CI, 1.61 to 1.90), 3.22 (95% CI, 2.98 to 3.49), and 1.00 (95% CI, 1.00) with adjustment of both age and gender, respectively. Age adjusted and gender specific IRR of treated group were 0.48 (95% CI, 0.47 to 0.50) for male and 1.00 for female. Gender adjusted and age specific rate of treated group were also highest in patient aged from 70 to 79 years (IRR, 1.29; 95% CI, 1.25 to 1.32) (Table 3).
Furthermore, 1,217 patients (2.5%) of hip fractures, 7,271 (5.2%) of spine fractures, and 188 (1.6%) of proximal humeral fractures received diagnostic bone density scans as well as osteoporosis medications (p < 0.001). IRR of group with proximal humeral fracture were the highest with adjustment of both age and gender (Fig. 3). Age adjusted and gender specific IRR of treated group were 0.43 (95% CI, 0.41 to 0.46) for male and 1.00 for female. Gender adjusted and age specific IRR of screened and concurrent treated group were also highest in patient aged from 70 to 79 years (IRR, 1.42; 95% CI, 1.35 to 1.49).
Younger (50–69 years of age) patients were less likely to be evaluated and managed for osteoporosis relative to older (≥ 70 years of age) patients (p < 0.001); and male was less likely to be evaluated and managed for osteoporosis relative to women (p < 0.001).
DISCUSSION
To our best knowledge, this is the first study to compare practice patterns in care of osteoporosis in the proximal humeral fracture with the other fractures in a large, population-based cohort that included almost 97% of the entire Korean population.
The current study demonstrated that the rate of diagnosis and treatment of the osteoporosis after fracture were low. Harrington et al.12) reported more than 20 percent of patients with hip fracture had not received any osteoporotic management in previous fracture. Panneman et al.13) also reported hospitalized patients for fracture remains less likely to be diagnosed and treated for osteoporosis. As shown in this data, especially middle aged male patients with proximal humeral fracture were the most easily underdiagnosed and undertreated for osteoporosis, as compared to any other factor. The present study also demonstrated that the evaluation and concurrent treatment of osteoporosis in proximal humeral fracture were lower than those of hip and spine. As the proximal humerus does not belong to the weight bearing area, physicians may underestimate the importance of management for osteoporosis of proximal humerus despite its increasing incidence. However, osteoporosis is one of the risk factors including age, anatomic reduction, and restoration of the medial cortical support for surgical failure in proximal humeral fracture.141516) Therefore, assessment of preoperative diagnosis for osteoporosis is essential for the treatment of proximal humeral fracture.
In this study, difference of the incidence rate between genders, which is related with sex hormone, was identified.1718) Estrogen deficiency is the major determinant of age-related bone loss in both sexes.17) Menopause in females causes much decrease in estrogen, which increases bone resorption up to 90%, while sex steroids in male decrease gradually. For the difference in incidence rate, physicians pay more attention to female osteoporosis than male in fracture. As a result, male osteoporosis is likely to be underestimated.31318) The current study confirmed that males were more underdiagnosed and undertreated than females for osteoporotic fracture.
The rate of diagnosis and treatment of osteoporosis in patients aged 50 to 59 years was lower than any other age group in this study. The Clinician's Guide to Prevention and Treatment of Osteoporosis by National Osteoporosis Foundation recommended diagnostic testing for osteoporosis in patients aged ≥ 50 years with low trauma fracture regardless of gender.19) However, physicians missed the opportunity to assess the bone density scan, because they regarded this age group too young for diagnosis of osteoporosis. Furthermore, due to the lack of universally accepted definition of low energy trauma,20) there might be confusion for the management of osteoporosis in terms of age. Thus, risk factor of patients with fracture should be evaluated with assessment tool to prevent overlooking or neglecting osteoporotic fracture by misinterpretation of low energy trauma in middle aged patients.
Orthopedic surgeon is more likely to be the first physician to take care of the patient with osteoporotic fracture in Korea. Their main concern appears to be reduction of fracture rather than management of osteoporosis. Lack of recognition and knowledge of orthopedic surgeon for the osteoporotic fracture may be one of the reasons.112122232425) Sorbi and Aghamirsalim25) reported that the typical orthopedic surgeon is not inclined to manage patients with osteoporotic fracture appropriately due to lack of knowledge in comparison with internist, which raised questions concerning their role in the management of osteoporosis. Several reports suggested that awareness of orthopedic surgeon reduces the risk of osteoporotic fracture and education is the way to improve management for osteoporosis.3102325) However, public management program could be a possible solution.51023) Singh et al.5) reported the screening and treatment for osteoporosis reduced the incidence of proximal humeral fracture by the osteoporosis prevention and management program.
The strength of the present study is that we investigated the rate of osteoporosis care in both male and female patients over the age of 50 years who had a fracture in a large, population-based cohort that included almost 97% of the entire Korean population. However, there are some limitations. First, we could not evaluate individual bone marrow density with T-score. Second, we distinguished low energy trauma from high energy trauma only by history of multiple fracture due to the limitation to access individual records.
In conclusion, the current cohort study indicated that the practice pattern for osteoporosis is inadequate for the diagnosis and treatment of patients with proximal humeral fractures. Physician should suspect osteoporosis in patients with proximal humeral fractures over the age of 50 years and provide appropriate knowledge-based care of osteoporosis after fracture. Several public programs and further studies are required to improve practice pattern for osteoporosis.


 XML Download
XML Download