

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Fanconi syndrome (also known as Fanconi's syndrome) is a disease of the proximal renal tubules of the kidney in which glucose, amino acids, uric acid, phosphate, and bicarbonate are passed into the urine, instead of being reabsorbed.1) Osteomalacia is the softening of the bones caused by defective bone mineralization secondary to inadequate levels of available phosphate and calcium.
Adefovir dipivoxil (ADV) is a commonly used antiviral agent in the treatment of chronic hepatitis B virus (HBV) or human immunodeficiency virus (HIV) infection. According to the literature, high-dose ADV therapy (60–120 mg/day) is nephrotoxic, whereas low-dose ADV therapy (daily dose of 10 mg) has been reported to be safe.23)
Although use of low-dose ADV therapy for chronic hepatitis B has been advocated in large clinical trials, several cases of hypophosphatemic osteomalacia due to Fanconi syndrome in patients receiving prolonged ADV treatment have been reported recently.4) However, a report of pathologic fracture induced by low dose ADV therapy is rare.
Here, we report a case of pathologic fracture of the femoral neck that developed in a chronic hepatitis B patient who was receiving prolonged ADV therapy at a dose of 10 mg daily.
CASE REPORT
A 43-year-old male presented in June 2011 with lower back and left hip pain, especially while bearing weight. The patient initially had dull and generalized aches. The pain then progressed to the lower back and left hip, which had developed 8 months and 3 months before the hospital visit, respectively and had aggravated since that time. He also had a history of right sixth rib fracture without a traumatic event 3 years before. He had chronic hepatitis B which was diagnosed 10 years ago and was prescribed lamivudine at the time of diagnosis. Lamivudine was changed to low-dose ADV daily after 3 years due to development of lamivudine resistance. He had no antecedent trauma or other medical history and was previously not taking any medication that is known to affect skeletal health or result in nephrotoxicity.
The patient showed an antalgic gait and mild tenderness on the lower back and left hip joint, but there was no abnormal finding on the physical examination, including the Patrick test and percussion test.
Laboratory investigations showed hypophosphatemia (1.0 mg/dL), mild hypokalemia (3.4 mmol/L), normocalcemia (8.5 mg/dL), and mild metabolic acidosis. He had normal levels of serum parathyroid hormone (29.36 pg/mL), 25-hydroxyvitamin D3 (27.5 nmol/L), and 1,25-dihydroxyvitamin D3 (46.7 pmol/L), but had mild renal impairment (estimated glomerular filtration rate, 61.75 mL/min) with upper limit of normal for serum creatinine (1.2 mg/dL). Thyroid function tests and serum levels of epinephrine, norepinephrine, and dopamine were within the reference range. Levels of bone turnover markers confirmed accelerated bone remodeling with a markedly elevated level of serum alkaline phosphatase of 314 IU/L (normal range, 40 to 160 IU/L), an increased serum osteocalcin level of 14.3 ng/mL (normal range, 4 to 12 ng/mL) and an increased urinary deoxypyridinoline/creatinine ratio of 12.08 nmol/mmoL (normal range, 2.4 to 5.4 nmol/mmoL). Liver function tests including hepatic enzymes, albumin, globulin, and bilirubin were within the normal range. HBV DNA level on quantitative PCR was below 20 IU/mL. Autoimmune serology for antinuclear antibodies, antineutrophilic cytoplasmic antibodies, anti-glomerular basement membrane antibodies and cryoglobulin was negative. Serum protein electrophoresis, free light chain kappa/lambda ratio, and peripheral blood smear result showed no evidence of multiple myeloma. Electrophoresis for alkaline phosphatase isoenzymes showed increased activity of bone fraction.
Urinalysis revealed significant glycosuria and proteinuria in the absence of hyperglycemia. Bone densitometry showed abnormally low bone mineral density with a mean lumbar T-score of –4.86 standard deviations and a mean lumbar Z-score of –4.69 standard deviations (lowest at L4 with a T-score of –5.57).
Plain radiographs of the chest, pelvis and hip joint showed no evidence of fracture or pathologic lesions (Fig. 1).
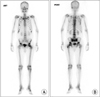
Whole body bone scintigraphy displayed increased uptake in the right sixth rib and left femoral neck area. Hot uptake in the right sixth rib was due to rib fracture which was diagnosed 3 years ago (Fig. 2).
Magnetic resonance imaging (MRI) revealed abnormal signals in both femoral neck areas. A significant dark line and signal changes were seen in the left femoral neck area on both T1- and T2-weighted images. A slight dark line was also observed in the upper portion of the right femoral neck. Based on these findings, pathologic fracture of the femoral neck was highly suspected, especially on the left side of the hip (Fig. 3).
Based on these results, a diagnosis of insufficiency fracture of the left femoral neck owing to hypophosphataemic osteomalacia in the context of Fanconi syndrome secondary to ADV therapy was made. Based on MRI findings and patient's symptoms, fixation of the left femoral neck with multiple cannulated screws was performed (Fig. 4). The suspected pathologic fracture of the right femoral neck was treated conservatively. ADV therapy was discontinued immediately after the diagnosis of acquired Fanconi syndrome was made and entecavir was prescribed at a daily dose of 1 mg. Elemental phosphate supplementation (2,722 mg/day), was started, and calcium carbonate (1,500 mg/day) and vitamin D3 (400 IU/day) were also prescribed.
The patient reported improvement in the symptoms 2 weeks after the treatment. Phosphate supplementation was discontinued after normalization of serum phosphate, 2 weeks after the treatment was started. At postoperative 6 weeks, the patient reported significant improvement in symptoms and ADL and returned to social activity. After 4 months of follow-up, normalization of hypokalemia, glycosuria and proteinuria and improvement in hypophosphatemia were observed.
After 14 months of follow-up, all laboratory test results, including those of blood and urine tests, were within the normal range and bone densitometry showed significant improvement in bone density (mean lumbar T-score: –1.4, lowest at L1 with a T-score of –1.8). The patient returned to previous social activity and follow-up X-ray of both femoral heads showed no signs of avascular osteonecrosis (AVN) (Fig. 5).
DISCUSSION
A number of therapeutic drugs are toxic to the renal proximal tubule and can cause the renal Fanconi syndrome. The most serious complications are bone demineralization from urinary phosphate wasting and progressive decline in kidney function.
Osteomalacia is a disorder of bone, characterized by decreased mineralization of newly formed osteoid at sites of bone turnover. Osteomalacia may be asymptomatic and can present radiologically as osteopenia. It can also produce characteristic symptoms, independently of the underlying cause, including diffuse bone and joint pain, muscle weakness, and difficulty walking. These symptoms may have an insidious onset. Bone pain is usually most pronounced in the lower spine, pelvis, and lower extremities, where fractures have occurred, and it may be associated with tenderness on palpation. The pain is characterized as dull and aching, and is aggravated by activity and weight bearing. Fractures may occur with little or no trauma, typically involving the ribs, vertebrae, and long bones.5)
These problems may be caused by various nutritional, medical, and surgical situations like malabsorption, gastric bypass surgery, celiac sprue, chronic hepatic disease, chronic kidney disease or toxic effect of drugs.
ADV is an orally bioavailable prodrug of adefovir that possesses potent in vitro activity against the HBV and the HIV. In general, drug toxicity in the renal proximal tubule is a dose-related phenomenon. ADV is excreted unchanged in the urine through glomerular filtration and tubular secretion and is known to be nephrotoxic at doses of 60 mg daily and above. Thus, the long-term safety of ADV, particularly nephrotoxicity, is a major concern in clinical trials. However, many clinical studies have shown that at a lower dose of 10 mg/day, ADV has a favorable risk-benefit profile with little or no evidence of renal toxicity after long-term therapy.23)
ADV-induced hypophosphatemic osteomalacia is a rare condition, but several such case reports have been published recently.46) Although it is generally believed that ADV 10 mg daily is not nephrotoxic with an incidence of renal events similar to that observed in the placebo group, ADV can be nephrotoxic even at low doses. For patients taking ADV, some reports recommend regular monitoring of renal function, calcium and phosphate levels. More frequent monitoring is needed in patients with pre-existing renal insufficiency.7)
Femoral neck insufficiency fractures are rare and are known to be associated with a variety of conditions such as vitamin D deficiency or renal dysfunction. In case of druginduced Fanconi syndrome, hypophosphatemic osteomalacia leads to a generalized defect in bone mineralization, causing excessive accumulation of undermineralized bone matrix and a lack of structural support for the periosteum. This generalized softening of the bone is associated with aches and pains in bones, muscles, and joints. These early signs of osteomalacia are often misdiagnosed as other conditions such as polymyalgia rheumatica, arthritis, or fibromyalgia. There are a number of published case reports of patients with spontaneous (atraumatic) femoral neck fractures, covering a range of etiologies. The femoral neck insufficiency fractures can become complete fractures if the symptoms and signs of hip injury are ignored. The consequences of a displaced femoral neck fracture can be devastating.
Majority of patients with osteomalacia induced femoral neck fracture are treated conservatively with bed rest and medical therapy. But some patients who have progressively worsening of fracture displacement are treated surgically.89)
Anatomically, femoral neck is an important passage for blood vessels that supply the femoral head and a pathologic fracture of this area can lead to disabilities resulting from severe pain and limited motion of the involved hip joint. Delayed diagnosis and inappropriate treatment can increase the possibility of avascular necrosis, and if displacement occurs, surgical treatment can be complex.10)
In our case, the patient's medical and medication history was taken thoroughly at the initial visit. Based on the patient's history and appropriate blood and urinary tests, early diagnosis of Fanconi syndrome was made and treatment was initiated early. With respect to the pathologic fracture of the femoral neck, early diagnosis established by bone scan and magnetic resonance (MR) imaging and early surgical treatment successfully prevented fracture progression and occurrence of AVN.
In conclusion, if a chronic hepatitis B patient who is receiving prolonged treatment with ADV complains of hip or back pain, early diagnostic studies related to Fanconi syndrome should be performed and additional radiologic evaluations such as plain X-ray, bone scan, dual energy X-ray absorptiometry, and MR imaging of the affected area should be performed to rule out pathologic fractures. As soon as the diagnosis of Fanconi syndrome is made, cessation of ADV and supplementation of elemental phosphorus and calcium should be carried out immediately to improve the symptoms of Fanconi syndrome. As delayed treatment of the pathologic fracture could lead to severe complications or burdensome operation, early immobilization and treatment should be performed to achieve reliable healing as soon as possible. The orthopaedic surgeons should be aware of osteomalacia and pathologic fractures caused by ADV administered as anti-HBV therapy.




 XML Download
XML Download