

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The changes of carpal alignment in malunion of distal radius fracture (DRF) are considered an adaptive response of the carpus to loss of normal architecture of the distal radius. In this situation, there are 2 types of carpal malalignment: (1) adaptive midcarpal malalignment, in which the proximal carpus angulates dorsally in line with the dorsally angulated articular surface of the distal radius and (2) pathologic radiocarpal malalignment, in which dorsal translation of the entire carpus occurs with respect to the distal radius.1) In radiocarpal malalignment, the lunate is usually observed in flexed position, in contrast to its extension posture in the more common midcarpal malalignment. In midcarpal malalignment, the adaptation of carpus at midcarpal level is usually improved after surgical correction of malunion of DRF. However, the effect of radial corrective osteotomy in the treatment of radiocarpal malalignment remains controversial. Verhaegen et al.2) and De Smet et al.3) noted that osteotomy of the distal radius could correct both types of carpal malalignment. However, Sennwald et al.4) reported that none of the patients with carpal instability showed a good result. We reported two cases of fixed lunate flexion deformity after a DRF, in which reduction and fixation of fresh fracture or corrective osteotomy of malunion to correct the lunate deformity showed no improvement in the fixed deformity.
CASE REPORTS
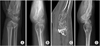
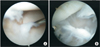
The first case was a 29-year-old pregnant woman presenting with a DRF. At the follow-up X-ray after closed reduction, an increase in the dorsal tilt of the radius and flexion of the lunate was observed; however, the operation was postponed because the patient was pregnant. At 8 months after the trauma, the patient complained of painful limited range of motion in the wrist. The preoperative dorsal tilt was 27° and the contralateral volar tilt was 7°. Corrective dorsal open wedge osteotomy of the distal radius was performed via volar approach to achieve the volar tilt of 3°, but flexion of the lunate persisted (Fig. 1). Arthroscopic examination, which was performed with hardware removal at postoperative 10 months, revealed cartilage denudation and fibrillation in the radiolunate joint (Fig. 2). Scapholunate and lunotriquetral ligaments were intact on arthroscopy.
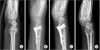
The second case was a 20-year-old woman with a distal radial fracture and an open volar triangular fibrocartilage complex rupture, who underwent immediate fixation with a volar locking plate and locking screws in the radius and repair of the triangular fibrocartilage complex. The postoperative volar tilt of the distal radius was 5° and that of the contralateral was 7°. Flexion of the lunate and dorsal subluxation of the carpal bones progressed even as early as several weeks after the operation (Fig. 3). The patient reported intermittent wrist pain. At 4 months postoperatively, an arthroscopic examination with removal of the plate and screws was performed and osteoarthritic changes in the radiolunate joint were identified (Fig. 4). No intraosseous ligament rupture was observed in arthroscopic examination.
DISCUSSION
Abnormal alignment and motion of the carpal bones leads to mechanical overload of the wrist joint, causing ligament attenuation and progressive dynamic instability.5) Bushnell and Bynum6) insisted that fixed intercarpal malalignment was a contraindication of radial corrective osteotomy. However, several studies reported the beneficial effect of radial corrective osteotomy in cases with carpal malalignment. De Smet et al.3) suggested that even though the alignment could not be completely restored, radial corrective osteotomy could have a significant effect on carpal realignment. McQueen and Wakefield7) reported that radial osteotomy could restore carpal alignment and improve function in 22 of 23 patients using nonbridging external fixator.
Verhaegen et al.2) suggested that incomplete correction of carpal alignment was due to incomplete correction of the dorsal tilt of the distal radius during radial corrective osteotomy. The dorsal tilt of the distal radius in our cases was restored to the volar tilt, but the correction was not achieved up to the average tilt of 10°, which might be the cause of remaining lunate flexion deformity. However, the volar tilt of the contralateral unaffected side in both cases was 7°, which implies that the surgical correction could have contributed to the remaining carpal malalignment despite no overcorrection.
Batra et al.8) indicated that failure of realignment after radial corrective osteotomy is related with extrinsic ligamentous derangement caused by incongruity of the articular facets of the radius. However, in our cases, computed tomography showed no gross bony abnormality including joint line incongruency or step-off. The arthritic changes such as cartilaginous wear and denudation in the radiolunate joint was observed only in arthroscopy. Both cases showed no rupture of the scapholunate and lunotriquetral ligament. Thus, fixed flexion deformity of the lunate might be associated with posttraumatic arthritic change in the radiolunate joint. Our case report highlights the need for added attention to injury of the articular surface of the radiolunate joint when a fixed lunate flexion deformity is found in a DRF.

 XML Download
XML Download