

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Various reasons have been cited in the difficulty involved for the removal of intramedullary nail after bone union. Direct manipulation can be attempted when a plate is used, since the implant is exposed. However, intramedullary nail inserted into the bone is difficult to operate on, as the implant is not exposed. So far, there have been few reports on the removal of an intra-articular nail in the tibia or femur, but no reports about nail removal in the ulna. The authors would like to report such a case, and the technique involved.
TECHNIQUE
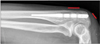
In February 2010, a 39-year-old man fractured both bones of the forearm after his arm was caught in a conveyor belt; he underwent a surgery at another hospital. An intramedullary forearm rod (Acumed, Hillsboro, OR, USA) was used in the ulna (Fig. 1). Nineteen months after surgery, an attempt was made to remove the implant; it failed because the threaded portion of the nail remover was broken while being connected to the nail (Fig. 1). Two years after the failed surgery, the patient visited us with complaints of occurrence of left elbow pain, without having any new trauma. A partial defect of the triceps tendon with severe pain and tenderness around the scar of nail insertion was noted. No other abnormalities were observed. Ultrasonography revealed partial rupture of the triceps tendon, and bursitis around the tender area. Based on these observations, the authors planned to remove the nail and repair the tendon.
Surgery was performed under general anesthesia, with the patient in the supine position; a tourniquet applied to the affected area. The forearm was placed on the patient's chest, with the shoulder joint and elbow joint each flexed at 90°. A longitudinal skin incision exposed the hole of the nail insertion and the interlocking screws. The inlet site of triceps brachii muscle was thinned not torn; it was not possible to grip since it was already covered by the bone. We removed the bone at the inlet site and created another bony window using an osteotome, to expose the interlocking screw holes. We inserted an impactor in the middle interlocking hole, after which we tapped the impactor towards the proximal side. The nail moved one inter-interlocking hole distance, and its end point passed through the triceps brachii tendon. We gripped the end point of the nail by a vise grip and used a hammer to remove it; however, the proximal part of the nail was damaged, and the vise grip and nail were separated (Fig. 2). This issue occurred recurrently. Finally, we hit the distal most part of the interlocking hole, and moved the nail to a two inter-interlocking hole distance. Subsequently, we could hold the nail precisely using the vise grip (Fig. 3), and were successful in removing the nail. The bony window was repaired using the stored bony segment. We finished the operation after repairing the triceps brachii tendon and the skin. Based on the authors' experience, we propose a surgical technique that can easily remove the nail, and minimize size of the bony window and damage to the triceps brachii.
Skin Incision
We recommend 2 skin incisions to minimize the total incision length. The distal incision is approximately the size of 2 inter-interlocking holes, and the proximal incision is about 1 cm, big enough to pass the nail (Fig. 4).
Bony Window
Only needs one inter-interlocking hole length of the bony window. It needs to be placed on the proximal 2 interlocking holes, and not on the distal hole (Fig. 5).
Intramedullary Nail Removal
In the bony window, an impactor is inserted on the distal hole, and tapped proximally by the mallet (Fig. 6A). When the hole is moved to proximal part of the bony window (Fig. 6B), a new interlocking screw hole appears in the distal part of the window (Fig. 6C). The impactor is then laid on the new distal interlocking hole and tapped again (Fig. 6D). In this process, the triceps brachii tendon can be carefully monitored, without being impacted by the nail in any way. The nail is then exposed enough to be gripped firmly (Figs. 3 and 6E). After the nail removal, the triceps brachii tendon is sutured and the bony window is covered, using the bone that was removed to make the window.
DISCUSSION
Intramedullary nailing can be used to treat fractures with minimal skin incision. Owing to its reliable biomechanical results, it is widely used in cases of long bone fracture. However, its direct placement into the bone can sometimes cause difficulty in handling. Incavo and Kristiansen1) reported on a method for removing the distal piece. A hooked-shaped, modified guide pin was used when the nail's middle portion had broken. Levy et al.2) reported a method of removing the distal piece of the broken nail, using another nail less than 1 mm. Georgiadis et al.3) reported on the management of failed proximal piece of the nail removal in the leg. Despite reports of such related cases, there were no case reports in the existing literature about failure of retrieval of an ulnar intramedullary nail. When the extraction device is broken during removal of the ulna nail, only a bony window the size of 2 inter-interlocking holes at the most proximal part of the nail can be used to remove the nail with minimal damage of the triceps brachii tendon and soft tissue. In spite of the simplicity and usefulness of this method, care should be taken when making the bony window, because there is potential risk of a fracture around the olecranon, especially in osteoporotic old patients.





 XML Download
XML Download