

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Vitamin D has an important role in calcium metabolism, bone health and musculoskeletal function. Normal vitamin D (25-hydroxy vitamin D) level is 30 ng/mL and > 30 ng/mL.1) Vitamin D and calcium deficiency cause osteomalacic myopathy, which could lead to increased body sway, decreased muscle strength, changes in gait, difficulties in rising from a chair and diffuse muscle pain.23) Low levels of vitamin D are associated with increased incidence of fall.45) Carpintero et al.6) showed poor functional recovery following hip fracture in elderly patients with low vitamin D. Nawabi et al.7) concluded that vitamin D levels positively correlate with both pre- and postoperative Harris hip scores in patients undergoing total hip arthroplasty (THA). Higher 25-hydroxy vitamin D concentrations are associated with better lower extremity function.8) But some studies have concluded that vitamin D does not affect functional performance,910) and postoperative recovery.1112) Unnanuntana and his colleague1112) reported that preoperative low vitamin D does not affect short term functional recovery after THA.
The effect of vitamin D levels on functional recovery after total knee arthroplasty (TKA) is unknown. Vitamin D deficiency is becoming a major concern worldwide, especially in postmenopausal osteoporotic women. Our aim was to study whether preoperative low vitamin D had any effect on functional recovery in patients undergoing TKA.
METHODS
We studied records of 214 TKA patients operated between October 2011 and April 2012. Of these, 120 patients with estimated preoperative vitamin D levels were included in the study. Serum vitamin D levels were checked in an early morning (overnight fasting) blood sample in all patients. All patients had primary osteoarthritis (OA) knee and had undergone unilateral TKA. We divided the 120 patients into two groups based on their preoperative serum vitamin D levels (25-hydroxy vitamin D levels), i.e., group 1 (deficiency group) with vitamin D levels < 30 ng/mL and group 2 (sufficiency group) with vitamin D levels ≥ 30 ng/mL. Accordingly, group 1 comprised 64 patients and group 2, 56 patients. Preoperatively, none of the patients had received vitamin D supplementation. All patients were supplemented with oral vitamin D (0.5 µg/day) from the 14th postoperative day for a duration of 4 weeks.
The same senior surgeon (RNM) performed all surgeries using computer navigation (Ci System; Johnson & Johnson, New Brunswick, NJ, USA). Skin incisions were midline, and midvastus arthrotomy was done for all patients. Posterior cruciate was sacrificed and PFC sigma series (Depuy Synthes, Warsaw, IN, USA) posterior stabilized implant was used in all cases. All patients also had the patellar component replaced using a 3-lug, all-polyethylene component. Cement was used for implantation in all cases. Patients were mobilized with a frame from the day after surgery and were generally discharged from the hospital on the fifth postoperative day. After discharge, patients were called for follow-up at 2 weeks, 6 weeks, and 3 months. We recorded body mass index (BMI) of all patients preoperatively. At 3 months, clinical data was collected for Western Ontario and McMaster Osteoarthritis Index (WOMAC), for Short-Form Health Survey (SF-12) questionnaire with Physical Composite Summary (PCS) and Mental Composite Summary (MCS), and for Knee Society Score (KSS) with Knee Score (KS) and Functional Score (FS). Radiographs were obtained pre- and postoperatively while the patient was in hospital, and subsequently at 3 months.
Statistical analysis of outcome measures between groups 1 and 2 was with two-sample t-test. Change in each outcome measure as adjusted for preoperative values was calculated and compared between groups using ANOVA.
RESULTS
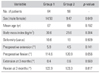
Of the 120 patients, 64 patients were group 1 (vitamin D deficiency) and 56 were group 2 (vitamin D sufficiency). Average age at surgery was 67 years in group 1 and 69 years in group 2 (p = 0.192) (Table 1). Of 64 patients in group 1, 50 were females and 14 were males; and of 56 patients in group 2, 47 were females and 9 were males. There was no statistical difference in the demographic parameters (age and sex) (Table 1). There was no statistical difference in preoperative and postoperative demographic parameters between groups (BMI, range of motion of knee joint, and deformity of knee joint [varus]) (Table 1).
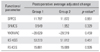
Preoperative and 3-month postoperative functional scores of both groups are presented in Table 2. These results show that SF-12 PCS (SFPCS), SF-12 MCS (SFMCS), KS-KSS, and FS-KSS scores remain comparable in both groups preoperatively and postoperatively with no statistical difference. Only the preoperative WOMAC score showed statistically significant difference (p = 0.040) between the two groups, the postoperative WOMAC score also showed no significant difference (p = 0.362).
The adjusted changes in these scores from preoperative to postoperative values are presented in Table 3. These results show that there was no significant difference in each score when its adjusted postoperative change in value over the preoperative value was compared between the two groups.
The results indicate that vitamin D deficient patients in group 1 had significantly poor functional status based on WOMAC score, as compared to vitamin D sufficient patients in group 2. However, the functional performance in both groups became similar at 3 months after TKA.
DISCUSSION
An important finding in our study was that patients with vitamin D deficiency had poor functional status preoperatively, as compared to vitamin D sufficient patients, based WOMAC score (p = 0.040). Several studies corroborate this finding. Serum vitamin D deficiency is associated with osteomalacic myopathy,3) which manifests in clinical symptoms that mainly include increased body sway, decreased muscle strength, changes in gait, difficulties in rising from a chair, inability to ascend stairs and diffuse muscle pains.23) Prevalence of low serum vitamin D levels is common among patients undergoing orthopedic surgery and may negatively impact patient outcomes in orthopedics.13) Vitamin D supplementation is associated with low mortality post-hip fracture.14) Bischoff-Ferrari et al.8) reported a significant positive association between vitamin D concentration and lower-extremity function in adult population. Lower-extremity function improved continuously with higher vitamin D concentrations.8) In a review article, Pfeifer et al.3) concluded that supplementation with calcium and vitamin D may improve muscle function.
The other important finding in our study was that at 3 months postsurgery, the functional performance was as good in vitamin D deficient patients as in vitamin D sufficient patients. In our study, all patients were supplemented with oral vitamin D supplements from the 14th postoperative day for a duration of 4 weeks postoperatively. This result indicated that knee arthroplasty should not be delayed in vitamin D deficient patients; rather, supplementation in the postoperative period is preferable to achieve comparable functional outcome at 3 months postoperatively. There are no other reports on the association between levels of vitamin D and outcomes after TKA for comparison with our findings. Nawabi et al.7) found that patients with vitamin D deficiency had lower postoperative Harris hip scores and were significantly less likely to attain an excellent outcome from THA; they concluded that vitamin D levels were positively correlated with both pre- and postoperative Harris hip scores. In their study, patients were not supplemented with vitamin D. Carpintero et al.6) reported a statistically significant relationship between reduced 1,25-dihydroxycholecalciferol levels and poor functional recovery at 1 year after sustaining hip fracture in their study. A multivariate analysis showed a significant relationship between 1,25-dihydroxycholecalciferol levels and absolute dependence of the patient 1 year after the fracture (p = 0.005).6) However, some studies concluded that low vitamin D status (25-hydroxyvitamin D < 30 ng/mL) did not adversely affect short-term function at 6 weeks after THA.1112) Unnanuntana and his colleague1112) concluded that there was no association between serum vitamin D levels and within–patient changes of score of each outcome measurement. Because a 6 week period is generally adequate to correct vitamin D deficiency, orthopedic surgeons can safely perform THA without delay and patients with low vitamin D levels should be treated once identified.1112)
Limitation of our study was its retrospective nature. Also, postoperative vitamin D levels at 3 months were not estimated. Hence, a record of post supplementation improvement in vitamin D levels was not available.
We concluded that knee osteoarthritis patients with vitamin D deficiency had poorer preoperative functions, as compared to vitamin D sufficient patients. However, if patients with vitamin D deficiency are treated postoperatively from 14th day for 4 weeks, the functional recovery at 3 months is comparable to patients with vitamin D sufficiency. Thus, TKA should not be delayed in vitamin D deficient patients; rather, supplementation during the postoperative period is preferable to achieve functional outcomes comparable to vitamin D sufficient patients.

 XML Download
XML Download