

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Femoral neck fracture is a common injury in the elderly, and its incidence is rising in parallel with an increase in traffic accidents and population aging. Arthroplasty and internal fixation can be viable surgical treatment options for those with femoral neck fractures. Internal fixation is the preferred treatment option if the patient is young and does not have very severely displaced fractures, whereas arthroplasty might be chosen over internal fixation if the patient is very old and has severely displaced fractrues.12) The incidence of avascular necrosis (AVN) and fixation failure following internal fixation of the femoral neck fracture was reported to be 20%–30% and 8%–15%, respectively.3)
Especially, a displaced fracture of the subcapital femoral neck is known to cause many complications, such as AVN of the femoral head or nonunion, compared with other femoral neck fractures.4567) The purpose of this study was to analyze the incidence of AVN and fixation failures in patients treated with internal fixation using cannulated screws after being diagnosed with subcapital femoral neck fractures.
METHODS
From January 1996 to January 2013, 853 patients were admitted to the Inha University Hospital with a femoral neck fracture. Based on the anatomic location, 214 patients were classified as having subcapital fracture. Of the 102 patients who underwent internal fixation using cannulated screws, 97 patients had a follow-up for more than 2 years. The cases excluded from the study were two cases of previous hip fracture, three cases with a history of cancer, eight cases with special medical conditions (one case of vasculopathy, two cases of pathological fractures, two cases of rheumatic arthritis, one case of osteomyelitis, two cases in chronic alcoholics) that may cause AVN. Finally, 84 patients were enrolled as subjects. Diagnosis of subcapital femoral neck fracture was performed by observing the fracture line at the junction between the femoral head and neck. We excluded lower transcervical femoral neck fractures from this study. Their ages when they first sustained fractures, fracture type graded by the Garden classification, the time elapsed before surgery, the degree of reduction after surgery, firm fixation after surgery, and the presence of osteoporosis were assessed. The Garden alignment index was used to assess the levels of reduction measured by plain radiography, which provided the anteroposterior (AP) and lateral views of hip joints immediately after surgery. When the Garden alignment index fell within the range of 160°–180° when seen on AP views and the range of 170°–190° when seen on lateral views, both images were declared as "excellent," as "good" if either of the two images fell within the range, and as "poor" if neither of the two images fell within the range. Two indices were used to assess firm fixation. As the first index, the average distance between the inserted fixation screws and the subchondral boundaries of the femoral head was measured using the AP and lateral views obtained by plain radiography. As the second index, whether or not the technique of 3-point fixation through the inferomedial cortical bone of the femoral neck was applied when seen on the AP and lateral views obtained by plain radiography. The cannulated screws were placed according to the '3 point principle.' Both ends of the screws were anchored in the firm bone (calcar femorale), the lateral femoral cortex and the subchondral bone of the femoral head, respectively.8) Using the two indices, cases in which the average distance to the subchondral boundaries of the femoral head was less than 10 mm and 3-point fixation was properly performed were declared as "excellent," cases in which the average distance was over 10 mm but the 3-point fixation status was deemed satisfactory, or the average distance was less than 10 mm but the 3-point fixation status was not deemed satisfactory were declared as "good," and cases in which the average distance was over 10 mm and the 3-point fixation status was not deemed satisfactory were declared as "poor." The average follow-up time of the patients was 36.8 months (range, 24 to 148 months).
A diagnosis of osteosynthesis was made when the trabeculation across the fracture line was observed on simple radiographs.9) A diagnosis of AVN was made when the patient reported clinically sustained pain in the hip joint during the follow-up period, with subchondral sclerosis or segmental collapse of the femoral head on simple radiographs.10) Fixation failure was defined by persistent pain in the hip joint without progression of fracture healing after a period of 6 months or redisplacement at the fracture site on simple radiographs.11)
Following spinal anesthesia, internal fixation was performed on all the patients using 6.5-mm cannulated screws upon completing anatomical reduction of the fractured site under C-arm. In case of impacted fracture, we tried to disengage the fracture anatomically as much as possible using the Steinmann pin or bone hook via the joystick technique. Antibiotics were administered for a minimum of 48 hours after surgery to prevent infection, and all the patients were instructed to avoid any weight gain during the following 6 weeks, and were subjected to an identical rehabilitation program during hospitalization.
The authors used IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA) program as a tool for statistical analysis. Wilcoxon rank sum test, Fisher exact test and multiple logistic regression analysis were used to statistically analyze the factors affecting the incidence of AVN and fixation failures.
RESULTS
The average age when the patients first sustained fractures was 55.8 years (range, 16 to 88 years). The average follow-up time was 36.8 months (range, 24 to 148 months), and the time elapsed before surgery was 2.8 days (range, 0 to 15 days).
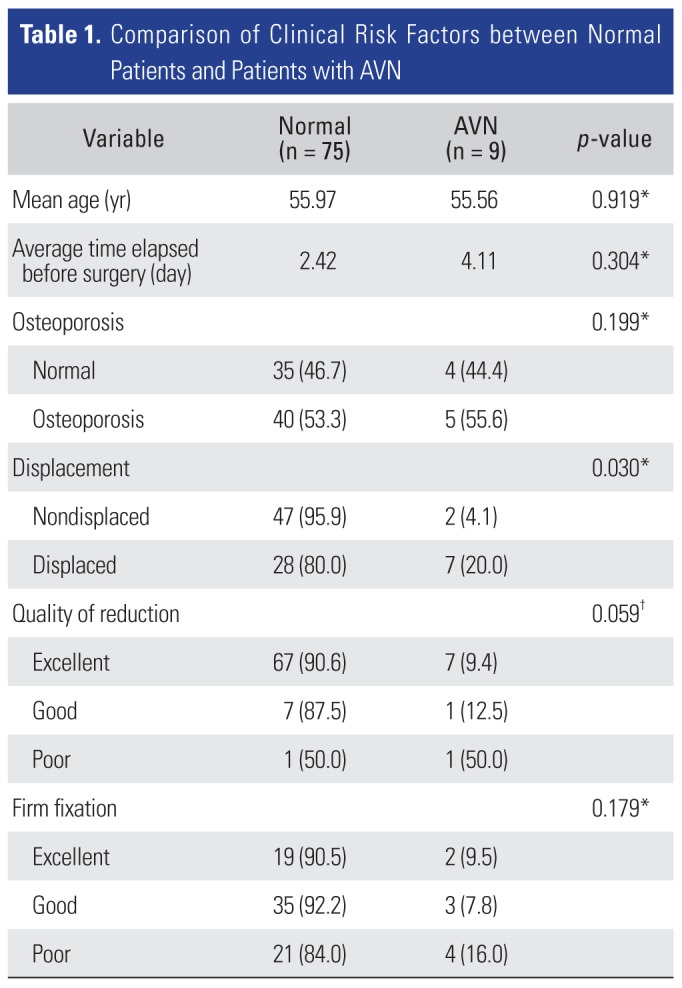
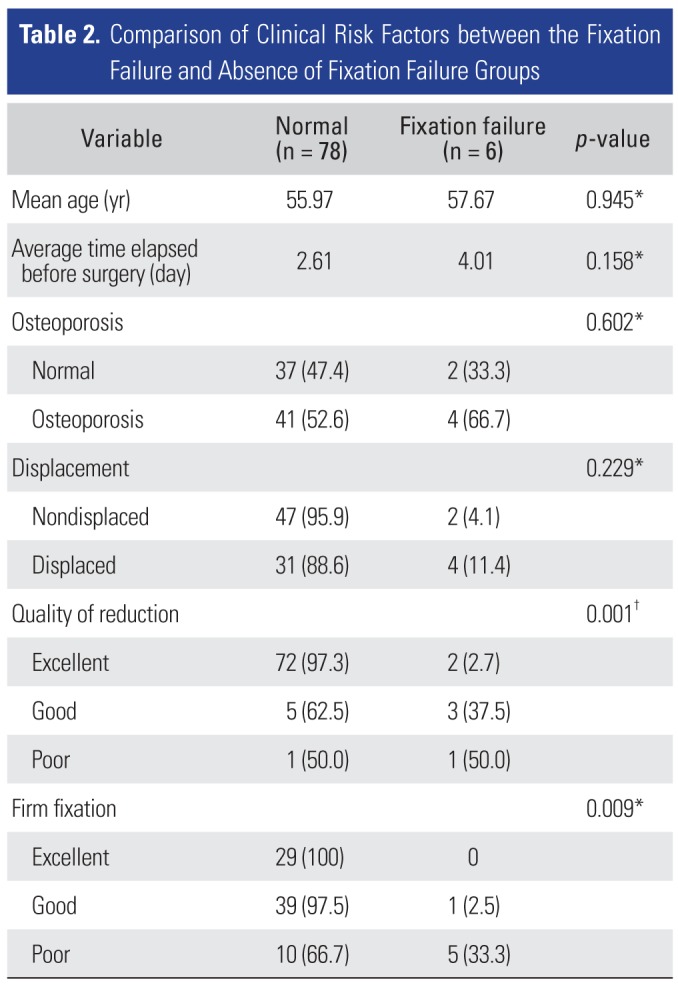
Of the 84 cases, nine cases (10.7%) showed AVN and six cases showed (7.1%) fixation failures, which were diagnosed as complications (Table 1). The average age of the absence of AVN group was 55.97 years, and the average age of the AVN of the femoral head group was 55.56 years, showing no statistically significant difference (p = 0.919). The average age of the absence of fixation failure group was 55.97 years, and the average age of the fixation failure group was 57.67 years, showing no statistically significant difference (p = 0.945) (Table 2). The average time elapsed before surgery in the absence of AVN group was 2.42 days, and the average time elapsed before surgery in the group with AVN was 4.11 days, showing no statistically significant difference between the two groups (p = 0.304). Of the total 84 cases, bone mineral density (BMD) evaluation was performed in 45 subjects who were over 60 years of age when they sustained fractures, and it was observed that osteoporosis was not an important factor in the development of AVN and fixation failure (p = 0.199 and p = 0.602, respectively).
Among the total 49 cases of nondisplaced fractures (types I and II), two cases (4.1%) with AVN of the femoral head were reported; among the total 35 cases of displaced fractures (type III and IV), seven cases (20%) with AVN were reported. Compared with the nondisplaced fracture group, the increase in the number of cases with AVN was statistically significant in the displaced fracture group (p = 0.030). Among the total 49 cases of nondisplaced fractures (types I and II), two cases of fixation failures (4.1%) were reported; and among the total 35 cases of displaced fractures (types III and IV), four cases of fixation failures (11.4%) were observed. Despite the rise in the number of fixation failures in the displaced fracture group over the nondisplaced fracture group, the increase was not statistically significant (p = 0.229). A 51-year-old woman visited Emergency Medical Center of Inha University Hospital for left hip pain after car accident. The Garden classification IV subcapital femoral neck fracture was observed. Firm fixation and quality of reduction was good. At postoperative 2 years, AVN of the femoral head was diagnosed (Fig. 1).
With respect to anatomical reduction after surgery, two cases of fixation failure (2.7%) were reported in the "excellent" group comprising 74 cases, three cases of fixation failure (37.5%) reported in the "good" group comprising eight cases, and one case of fixation failure (50.0%) in the "poor" group comprising two cases. The poor reduction status after surgery was related to fixation failures (p = 0.001).
With respect to firm fixation after surgery, the poorer the firm fixation condition, the higher the incidence of AVN; however, the results were not statistically significant (p = 0.179). No case of fixation failure (0%) was found in the "excellent" fixation condition group, and one case of fixation failure (2.5%) and five cases of fixation failure (33.3%) were reported in the "good" fixation condition group comprising 40 cases and the "poor" fixation condition group comprising 15 cases, respectively; the poorer the firm fixation condition, the higher the incidence of fixation failures. This increase was statistically significant (p = 0.009). A 68-year-old man visited Emergency Medical Center for right hip pain after a 1.5-m fall down. Firm fixation was poor, but quality of reduction was good. At postoperative 1 year, fixation failure was diagnosed (Fig. 2).
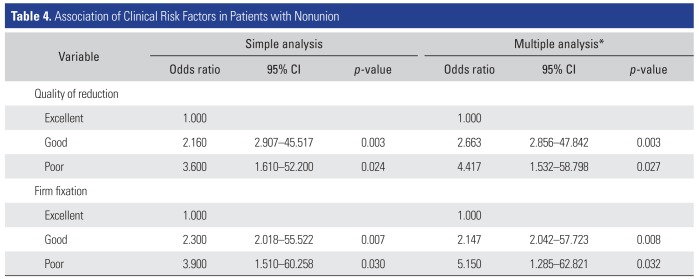
As indicated previously, the presence of displacement was significantly related to the incidence of AVN. The authors conducted a multivariable analysis using multiple logistic regression test and confirmed that there was a statistically significant increase in the incidence of AVN as the degree of displacement became more severe (Table 3). We also studied the relevance of quality of reduction and firm fixation with the incidence of nonunion using multivariable analysis and concluded that there was a statistically significant decrease in the incidence of fixation failure with better quality of reduction and firm fixation (Table 4).
DISCUSSION
Although the incidence of femoral neck fractures increases in proportion to the increase in average life expectancy, these fractures are not fully treatable and are associated with complications that are not significantly reduced in number.4) Despite the fact that recent studies have shown accurate anatomical reduction, fixation stability, and the time elapsed before surgery as factors correlated with the incidence of complications,121314) the existence of a slew of counter arguments at this point is making the issue of finding right treatments controversial.3151617)
Subcapital femoral neck fracture is considered to cause many complications, such as AVN or fixation failure, compared with other femoral neck fractures.4567) On the other hand, there is a report that the location of the intracapsular fracture does not affect the management or outcome.18) The incidence of AVN after fixation was reported to be as high as 10%–25%.192021)
In this study, the incidence of AVN in the nondisplaced fracture group was 4.1% and the incidence of AVN in the displaced fracture group was 20%. The high incidence rates of AVN caused by displaced fractures were statistically significant in comparison with the incidence rates of AVN caused by nondisplaced fractures. Our data support the claim that the degree of displacement of fracture is likely to have a major impact on the incidence of AVN.1422) However, the incidence of fixation failures in displaced fractures was not statistically significant, compared with the incidence of fixation failures in nondisplaced fractures. According to other previous studies, reduction accuracy has a huge impact on prognosis.323) The low rate of AVN in cases in which anatomical reduction was properly performed, as compared to the rate of AVN in cases in which anatomical reduction was improperly performed, was statistically significant; however, no statistically significant difference in the incidence rates of AVN was found in this study. This is thought to be because of the difficulty in showing statistical significance due to the rarity of cases with improperly performed reduction in this study; and it is thought that the rarity of improper reduction might be attributable to the performance of arthroplasty in the first place when anatomical reduction was not a viable option and anatomical reduction was properly performed in most patients of this study and issues regarding reduction accuracy which are already known as key factors in prognosis.
The relationship between the timing of surgery and complications has been the subject of many studies, 2425) and has remained a contentious issue. Jain et al.24) compared early fixation (within 12 hours of injury) with delayed fixation (more than 12 hours after injury) and recorded an incidence of AVN of 16% in the delayed fixation group compared with an incidence of AVN of 0% in the early fixation group. However, according to other studies, the time elapsed between the occurrence of femoral neck fractures and surgery has no definitive impact on the risk of AVN.4) In addition, some studies report that the impact of the time elapsed between fracture occurrence and surgery on the risk of AVN is unclear.16) The results of this study were largely in line with the results of a recently published study, in which the temporal difference (from fracture occurrence to surgery) between the groups with and without AVN after internal fixation was not found to be statistically significant (p = 0.304).
Although a patient's bone density, which is critical for fixation safety after internal fixation,26) is also known to have an impact on prognosis, whether osteoporosis is related to the risk of AVN or fixation failure was clarified in a statistically significant manner in this study. The reason for this is that the majority of patients with subcapital femoral neck fractures in this study were relatively young; of a total of 84 subjects, BMD evaluation was only performed in 45 patients aged over 60 years; and only 40 of them were diagnosed with osteoporosis, making it difficult to show statistical significance in number due to the small sample size.
Further implications of this study are that it analyzed the incidence of complications of subcapital femoral neck fractures-which has not received much attention and has not been studied extensively-after internal fixation. In general, femoral neck fracture is known to be a common injury in elderly osteoporotic women. However, unlike other fractures, subcapital femoral neck fractures are common injuries in younger age groups, and the average age of the patients in this study was 55.8 years when they sustained fractures. Internal fixation is usually preferred over arthroplasty due to its ability to preserve the femoral head, and the fact that prosthetic replacement can only be used for a limited amount of time; however, if a patient develops complications after internal fixation, it would be incorrect to force the patient to undergo arthroplasty as a secondary treatment because of the complications. Therefore, it can be said that assessment of such risk factors is worthwhile in this regard.
The small number of patients included in this study in absolute terms might limit the application of the study results given the relative rarity of subcapital femoral fractures in comparison with other types of femoral neck fractures and the performance of arthroplasty in many patients who are very old or have severely displaced fractures. In addition, BMD evaluation was not performed in all the patients because of the high number of patients aged under 60 years; thus making it difficult to accurately assess the impact of osteoporosis on the incidence of complications. However, as the risk of complications of subcapital femoral neck fractures is lower than that thought previously, internal fixation can be considered in a proactive manner if the patient is not very old and does not have a very severely displaced fracture.
In conclusion, the rates of AVN and fixation failures after internal fixation using cannulated screws after patients sustain subcapital femoral neck fractures were 10.7% and 7.1%, respectively. The complication rates for subcapital femoral neck fractures were lower than those previously reported; hence, internal fixation could be a primary treatment option for these fractures.



 XML Download
XML Download