

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The population of patients over 90 years of age (nonagenarians) has experienced the fastest growth in recent years. Americans 95 years and over alone experienced an increase in over 25%, from 337,000 to 425,000 between 2000 and 2010.1) This population is at high risk for falls and resulting fractures. Furthermore, due to their age some physicians may be hesitant to operate surgically on > 90-year-old patients.
Recently, evidence has suggested surgical treatment for nonagenarians often results in satisfied patients and is prudent.234) Other studies have compared the outcomes of nonagenarians to younger patients, generally showing worse outcomes for the older cohorts.56) However, few studies have examined the parameters affecting nonagenarian patient outcomes providing physicians with information to make decisions as to when outcomes are likely to be positive.
In addition nonagenarian patients frequently suffer from comorbidities and functional impairment, which can have significant effects on operative outcome.789) As the number of fractures occurring in nonagenarian patients increases, preoperative factors that might affect the outcomes are vital for surgeons to be aware of.
The aim of this study is to report the mortality rates as well as functional outcomes following hip surgery in patients over 90 years of age presenting with a hip fracture. Furthermore, we assessed the efficacy of the Deyo index comorbidity scoring system in predicting the before-mentioned outcomes.
METHODS
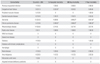
A retrospective chart review was performed to determine outcomes of nonagenarian patients (over 90 years of age) who underwent operative hip fracture repair between January 1st, 2009 and August 21, 2013 at a level 1 trauma center. Institutional Review Board approval was obtained before chart review began. Patients who were treated conservatively, underwent a girdlestone procedure, or resided in a different state than the institution were excluded. This led to a total of 39 patients with a mean age of 93.3 ± 2.3 years being included in this study (34 females, 5 males) (Table 1). Twenty-six patients (66.7%) had trochanteric fractures and were treated with sliding hip screws. The remaining 13 patients (33.3%) suffered femoral neck type fractures; 11 of those received a hemiarthroplasty and 2 underwent internal fixation with cannulated cancellous screws.
Patient comorbidities were quantified using the index described by Deyo et al.10) The Deyo index assigns scores of 1 to 6 for 17 possible comorbidities (Table 2). Patients with a cumulative score of 1 to 4 are considered to be moderately comorbid and patients with a score greater than 5 are considered to be severely comorbid. Accordingly, our cohort was divided into 3 groups: three patients (7.7%) had a Deyo score of 0, 27 (69.2%) were moderately comorbid, and nine (23.1%) were severely comorbid.
The investigated outcomes in this study were mortality, return to prefracture living arrangements, postoperative level of mobility, 90-day readmission rates and length of hospital stay (Table 1). In-hospital, 90-day, 1-year, and overall mortality rates were calculated. Living arrangement possibilities included home, assisted living, nursing home, and hospice in order of increasing intensity of care. Patients were assigned as resuming previous living arrangements or being moved to a living arrangement with more intensive care. Regarding mobility, patients were assigned as mobile if they were walking unaided or used a cane or walker postoperatively. Patients who were confined to a wheelchair or bedridden were considered immobile.
Statistics
All analyses were performed using the IBM SPSS ver. 21.0 (IBM Co., Armonk, NY, USA). Survival was analyzed by the Cox proportional hazards regression model. The chi-square test was used for the analysis of nominal variables. Nonparametric continuous variables were tested by the Mann-Whitney U-test, while parametric variables were tested by an independent sample t-test. Prediction analysis was performed by binomial logistic and multiple regres sion models on dichotomous and continuous variables, respectively. Whenever a covariate was found to be statistically different among an investigated group, it was placed as a predictor variable in the regression model in order to be controlled for. The level of significance was set at p < 0.05 for all comparisons.
RESULTS
Overall, four patients (10.3%) died in-hospital predischarge, eight (20.5%) within 90 days of surgery and 14 (35.9%) within 1 year. In-hospital death was due to myocardial infarction in three patients (8%) and pneumonia in one patient (3%) (Table 3). Additionally, in the direct postoperative period, two patients developed superficial wound infections, which were treated with multiple wound dressing changes and did not require further intervention. Within 90 days, additional four patients expired due to pneumonia in two patients (5%) and myocardial infarction in the remaining two (5%). At the 1-year time point, additional six patients expired, four (10.3%) due to myocardial infarction and two (5%) due to complications of renal disease. Return to previous living arrangement was achieved in 24 patients (61.5%), while mobility was regained in 19 patients (48.7%). Six patients (15.4%) were readmitted within 90 days postoperatively. Of those six readmitted patients, three (8%) had cardiac events, two (5%) suffered pneumonia, and one (3%) had complications of renal disease. The mean duration of hospital stay was 8.5 ± 6.4 days (range, 0 to 27 days) (Table 1).
No statistically significant correlations could be detected between Deyo level (no comorbidities; moderately comorbid; and severely comorbid) and the in-hospital (p = 0.37), 90-day (p = 0.65), or 1-year (p = 0.97) mortality rates. Additionally, no statistically significant correlations were observed between Deyo level and return to preoperative living arrangements (p = 0.9), mobility (p = 0.18), 90-day readmission (p = 0.64), or length of hospital stay (p = 0.68).
In-hospital mortality survival analysis demonstrated a hazard ratio (HR) of 0.089 (confidence interval [CI], 0.009 to 0.86; p = 0.036) and 0.143 (CI, 0.02 to 0.94; p = 0.047) for congestive heart failure (CHF) and chronic pulmonary disease (CPD) patients, respectively. These HRs indicate that the probability of dying in-hospital was reduced by 91% (p = 0.036) and 86% (p = 0.047) in patients without a history of CHF or CPD, respectively.
Ninety-day mortality survival analysis demonstrated an HR of 0.121 (CI, 0.024 to 0.6; p = 0.01) and 0.189 (CI, 0.045 to 0.8; p = 0.024) for dementia and CPD patients, respectively. These HRs indicate that the probability of dying within 90 days postoperatively was reduced by 88% (p = 0.01) and 81% (p = 0.024) in patients without a history of dementia or CPD, respectively.
One-year mortality survival analysis demonstrated an HR of 0.252 (CI, 0.087 to 0.73; p = 0.01) and 0.221 (CI, 0.068 to 0.86; p = 0.01) for dementia and CPD patients, respectively. These HRs indicate that the probability of dying within 1 year postoperatively was reduced by 75% (p = 0.01) and 80% (p = 0.01) in patients without a history of dementia or CPD, respectively.
Furthermore, dementia patients were 6.1 times (CI, 1.2 to 31.1; p = 0.029) more likely not to return to previous living arrangements. Interestingly, dementia patients were also found to have stayed on average 5.3 days less (p = 0.013) in the hospital when compared to nondementia patients. This observation was included in the binomial regression analysis model for the dementia group in order to be controlled for.
DISCUSSION
An in-hospital mortality rate of 10.3% was calculated for our study. Reported in-hospital mortality rates of nonagenarian patients vary depending on the type of fracture and from study to study, but have recently shown to range from 5.0% to 10.0%.6111213) Furthermore, our 10.3% inhospital mortality rate is in agreement with the 9.9% 30-day mortality rate in a recently published study by Lin et al.14) on the short-term outcomes of surgically treated hip fractures in nonagenarians. However, our overall 1-year mortality rate nearly doubled that reported by Lin et al.;14) we suspect that one of the factors influencing their superior results may be the fact that they lost more than 25% of their patients to follow-up during the first postoperative year. We also speculate that another factor might be that their patient cohort stayed longer in-hospital (12.4 days) postoperatively relative to our patients (8.5 days). We will explain later in the discussion why we believe a shorter postoperative in-hospital stay might affect mortality and how dementia might play a role.
Comorbidity indexes may be used to predict overall success following surgery and return to normal function; however, many require careful review of medical records which may be time-consuming. This is particularly true for nonagenarian patients who often have decades of medical records. We propose an efficient screening of nonagenarians presenting with trochanteric and femoral neck fractures to assess for surgical risk and likely outcome. Our screening involves assessing for dementia, CHF, and CPD. We consider those to be the 3 most important comorbidities for presurgical screening in the nonagenarian population undergoing hip fracture repair.
CHF is generally accepted as a significant predictor of perioperative cardiac complications. We found this to be true for the nonagenarian population as well. Heart failure is an important complication following non-cardiac surgery.1516) In our study, nine patients (23.1%) presented with a history of CHF. CHF displayed a significant correlation with perioperative mortality. A third of the patients with CHF expired in hospital. A trend was also found between CHF and failure to regain mobility postoperatively, but this did not achieve statistical significance (p = 0.07). Patients and their families should be made aware of the potential negative impact that CHF might have on the postoperative outcomes.
Forty percent of CPD patients in our cohort died in hospital predischarge versus only 5.9% of non-CPD patients. Our finding is consistent with that of previously published large study conducted on hip fracture patients in Sweden which concluded that patients with chronic obstructive pulmonary disease (COPD), which is one of the most common chronic lung diseases, have a 60%–70% higher risk of death following hip fracture relative to those without COPD.17)
Dementia was also identified, as it was the second most common comorbidity encountered in our study (n = 13, 33.3%). In addition, all 4 in-hospital mortalities had suffered from dementia. Dementia is especially prevalent among the nonagenarian population. Mini mental status exam (MMSE) scores of patients ≥ 85 of age varies based on educational level, but the average is 24.18) An MMSE score of < 24 is indicative of dementia or delirium. Hence, it is expected that nearly 50% of nonagenarian patients will present with some form of cognitive impairment. Besides prevalence, it has also been suggested that patients with dementia have lower motivation to rehabilitate following surgery and lower rates of recovering walking ability.1920) Postoperative ambulatory level has been demonstrated to impact 1-year mortality and is important for survival rate.21) Our results indicate similar inferior outcomes regarding return to previous living arrangements and the 90-day and 1-year mortality rates in dementia patients. For these reasons, we believe dementia is an important predictor of rehabilitation success. A rather interesting observation that we found in our cohort is that dementia patients had a shorter postoperative length of stay in the hospital. A recently published large study conducted on hip fracture patients demonstrated that a shorter length of stay was associated with an increased risk of death after hospital discharge.22) The probable reason behind the shorter length of stay of our dementia patients remains unknown. Even though we successfully controlled for this variable in our regression model, it still might have confounded our results regarding the dementia patients. Therefore, further research regarding dementia patient's postoperative length of stay is warranted in order to investigate another potential reason behind the inferior outcomes observed in this patient category. History of dementia is relatively easy to assess, but it is important to not confuse delirium with dementia. Delirium is an extremely common problem seen in the elderly especially with hip fractures. It is estimated that delirium occurs in up to 61% of elderly patients with hip fractures.23) Here family questioning about patients' mental state prior to injury is extremely useful and important for differentiating between dementia and delirium.
In conclusion Deyo scores were not statistically significant in predicting postoperative outcomes following hip surgery in patients over 90 years of age. However, dementia, CHF and CPD, which are 3 of the 17 comorbidities included in the Deyo index scoring system, demonstrated statistically significant correlations with inhospital, 90-day and 1-year mortality rates. We observed that dementia patients had shorter hospital length of stay relative to nondementia patients. Are dementia patients in general being discharged earlier than others or was this just a coincidence in our research group? Unfortunately, due to the small size of our study, we could not reach a conclusion regarding this observation. Therefore, further research investigating the extent and effect of this observation on the outcomes following hip surgery in dementia patients is warranted.


 XML Download
XML Download