

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Total knee arthroplasty (TKA) has been shown to have a success rate of 90% at 10 years postoperatively. This has greatly improved the quality of life of patients with late knee joint arthritis. However, in recent years, the incidence of TKA and its resulting complications have greatly increased.12) Deep infection is one of the most serious complications, with a reported incidence of 0.5%-5%.34) The prophylactic use of antibiotics, advances in surgical techniques, and improvements of the surgical environment have greatly reduced deep infection rates; however, the incidence of infections after TKA is increasing, proportionate with the increase in the frequency of TKA.56)
In cases of chronic deep infection after TKA, a two-stage revision arthroplasty has been recommended as an optimal treatment modality, and has been reported to have a success rate exceeding 90%.67) A cement spacer is used during the first stage of revision arthroplasty; these spacers can be classified as articulating and non-articulating. The latter type restricts the range of motion after first-stage revision arthroplasty, and is thus effective for controlling infections. However, it prevents joint movements until the second stage, and thus, increases patient discomfort. Due to soft tissue contracture, an additional surgical procedure, such as resection of the quadriceps femoris muscle or tibial tubercle osteotomy, may be required during revision arthroplasty.89) To resolve this, an articulating cement spacer has been developed that allows the patient to perform joint movements to some extent before the second-stage revision arthroplasty, thus also preventing soft tissue contracture.1011) Moreover, it has been reported that in terms of controlling infection, there is no significant difference between a non-articulating and an articulating spacer.121314) Various kinds of articulating spacers have been introduced, and surgeons differ regarding the type of articulating spacer to be used: metal-on-polyethylene, cement-on-cement, or cement-on-polyethylene spacers.
Given the above background, the authors performed a two-stage revision arthroplasty using a novel articulating metal-on-cement spacer. This paper describes the treatment outcomes, and includes a review of the literature.
METHODS
Study Patients
Approval of the ethics committee of the Institutional Review Board of Kyungpook National University Hospital was obtained for this retrospective study (IRB number: 2013-06-016). From January 2007 to June 2011, 25 patients (26 cases) underwent a two-stage revision arthroplasty using mobile cement prosthesis at our institute, after receiving a diagnosis of chronic infection post TKA. Of these, 19 patients (20 cases), with a minimum follow-up of two years, were enrolled in this retrospective study. This clinical series consisted of 16 women and 3 men, having mean age 71 years (range, 63 to 75 years). Mean follow-up was 29 months (range, 24 to 49 months). Primary TKA was performed with a diagnosis of degenerative osteoarthritis. Other underlying diseases at index surgery were hypertension (13 cases), diabetes mellitus (8 cases), and renal failure, asthma, tuberculosis, or cerebral infarction (1 case each).
To diagnose infection after TKA, the presence of swelling, erythema, and heat sensation were checked by a physical examination. We also determined whether the patients presented with clinical symptoms, such as pain and tenderness. Laboratory tests included complete blood count, white blood cell (WBC) count, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). In addition, radiography, joint fluid cell counts, blood culture, intraoperative findings, histopathologic findings of synovial membranes, and culture results were considered. Based on the results obtained, a diagnosis of infection after TKA was established. In this series, the pathogenic bacteria were identified in 9 cases by culture; these included 3 cases of methicillin-sensitive Staphylococcus aureus, 2 cases of methicillin-resistant S. epidermidis, 2 cases of α-hemolytic streptococcus, 1 case of methicillin-resistant S. aureus (MRSA), and 1 case of Escherichia coli (Table 1).
Operative Technique
All surgical procedures were performed by a single orthopedic surgeon (HSK). During the first-stage of revision, a medial parapatellar approach was used, and access was via the previous surgical scar. Necrotized bone, soft tissue, and synovium presumed to be infectious were all removed. If possible, en bloc resection was performed, and this was followed by histopathologic examination and culture of the resected soft tissue and synovium. Using an osteotome, the polyethylene, femoral, tibial, and patellar prostheses were removed and complete debridement of the intramedullary region, which was presumed to be infected, was performed. These procedures were followed by massive irrigation with normal saline.
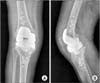
Using an osteotome, all cement components attached to the femoral prosthesis were removed as much as possible, after which they were washed and autoclaved at 132℃ for 30 minutes. A pack of cement was then mixed with antibiotics, and this cement paste was applied to the autoclaved femoral prosthesis, which was subsequently fixed to the femur. Another pack of antibiotic-impregnated cement was prepared and inserted in the tibia at a thickness that maintained the knee joint gap. Beads were also inserted in the intramedullary canal, if needed. To achieve joint congruency, a deep dish-like molding was made intraoperatively, by flexing and extending the knee joint. If the causative bacteria had been identified preoperatively, appropriate antibiotics were mixed with the powder component of the bone cement; however, if no causative bacteria were identified, a pack of cement (40 g) was mixed with vancomycin (4 g) and first-generation cephalosporin (4 g) before application. The bone cement used was Refobacin (Biomet Orthopaedics, Ried B. Kerzers, Switzerland), which contained 0.5 g gentamicin per pack (Figs. 1,2,3,4,5).
After the first revision stage, drainage was maintained for 3-5 days and splinting for a week, during which time the pain was managed with medication. Thereafter, passive joint movement was performed using a continuous passive motion unit, and this was accompanied by active joint movement. At 2 weeks postoperatively, patients were gradually allowed to perform gait tasks with partial weight-bearing. It was recommended to use a knee orthosis during weight-bearing. Before the sample culture test results were acquired after the first-stage revision, suitable antibiotics were administered, based on the bacterial strains identified in joint aspirates obtained prior to hospitalization. Thereafter, these were replaced with suitable antibiotics after obtaining the intraoperative culture and sensitivity results, and consultation with a board-certified specialist in infectious diseases. If no causative bacterium was identified, empirical antibiotics were used. Antibiotics were administered by intravenous injection for 4-6 weeks.
Second-stage revision arthroplasty was conducted based on the current, and later the systemic, status of the patient. The factors considered were: ESR had decreased, CRP had normalized (at < 0.5 mg/dL), complete blood WBC count had normalized, and no sign of infection was evident by clinical examination. Second-stage revision arthroplasty was also performed via the previous surgical scar. Initially, soft tissue and synovium around the joint were biopsized, and if the number of multinuclear leukocytes by frozen section biopsy was < 10 at high magnification, it was considered that no acute inflammation was present.
During second-stage revision arthroplasty, metal blocks, cement prosthesis, and an allobone graft were used to restore the bone defects. A cruciate ligament-substituting knee prosthesis and a constrained type knee prosthesis were used in 12 and 8 cases, respectively. Cement was used to fix the prostheses; it was prepared by mixing appropriate antibiotics with the cement powder component if causative bacteria had been identified, and if not, a pack of cement (40 g) was mixed with vancomycin (1 g) and first-generation cephalosporin (1 g).
Clinical Assessments
Range of motion was determined prior to the first and second stages of revision arthroplasty, and at the last follow-up. In addition, Hospital for Special Surgery (HSS) knee scores and Knee Society (KS) knee score and functional score (FS) were determined after the two surgical stages. After second-stage revision arthroplasty, plain radiography was performed at 2 weeks, 3 months, and 6 months, and later annually. To evaluate the degree of joint contracture between the first stage and second stage, the authors used the frequency of rectus snip during second-stage revision arthroplasty. In addition, patients were also examined during follow-up for complications or infection recurrence.
Student t-test was used to analyze parametric continuous data. Statistical significance was accepted for p-values of < 0.05. IBM SPSS ver. 21 (IBM Co., Armonk, NY, USA) was used for all analysis.
RESULTS
A total of 20 knee surgeries were studied: 7 had undergone primary TKA at Kyungpook National University Hospital, and 13 at another institution. A mean of 35 months (range, 2 to 132 months) had elapsed before the prosthesis was removed from the onset of infection, and the mean time between the first and second stages of revision arthroplasty was 25 weeks (range, 4 to 116 weeks).
The mean range of motion of knee joints was 70° (range, 15° to 100°) prior to first-stage revision, 72° (range, 40° to 120°) prior to second-stage revision arthroplasty, and 113° (range, 90° to 135°) at final follow-up, indicating a significant improvement following revision arthroplasty (p < 0.05). However, no significant difference in mean range of motion was observed after the first stage (p = 0.703). There were no occurrences of fracture of the cement spacer during the interim in-between stages.
Mean HSS score was 40 points (range, 5 to 68 points) prior to the first stage and 86 points (range, 56 to 100 points) at the final follow-up (p < 0.05). The mean KS knee score and FS were also significantly increased from 43 to 82 and from 30 to 54, respectively (p < 0.05).
On the final follow-up radiographs, only 1 patient with a recurrent infection exhibited a radiolucent line and osteolytic lesion. In this case, extensive muscle necrosis and a severe abscess were observed on gross examination during the first-stage revision surgery. Two months after the second stage, this patient presented with a recurrence. Two-stage revision arthroplasty was re-performed, and the infection was controlled.
There were only 2 cases of postoperative complications. Both cases were deep vein thrombosis in small-sized veins distal to the knee joint, which were detected using a 64-channel multidetector row computed tomography-indirect venography.15) Both cases were treated using mechanical treatment modalities, such as active joint movement and pneumatic pump therapy.
No patient required a resection of the quadriceps femoris (rectus snip) or tibial tuberosity osteotomy, which is routinely performed for joint access in cases of joint contracture.
DISCUSSION
In this study, the two-stage revision arthroplasty involves recycling of the femoral prosthesis after removal from the infected knee joint, and implantation of a mobile prosthesis by intraoperative molding of antibiotic-impregnated cement; this technique provided an excellent clinical and radiological outcome.
A two-stage TKA can be performed using an articulating or a non-articulating spacer, although it has been suggested that a non-articulating spacer is likely to be more effective at controlling infections, based on the outcomes of infected joint stability.4) However, it causes great discomfort due to limited range of motion prior to the second-stage surgery; also, due to soft tissue contracture around the knee joint and the quadriceps femoris, the surgical approach is more difficult during the second stage.41617) An articulating spacer has been developed to resolve the disadvantages of the non-articulating spacer, thus making it possible for patients to perform joint movements between the first and second stages of revision, which in turn reduces discomfort and prevents soft tissue contracture. Thus, this spacer simplifies the surgical approach during the second stage and produces excellent functional outcomes. Several comparative studies have also reported that use of an articulating spacer is more effective in infection control.71018)
Articulating spacers can be classified by their joint surfaces as metal-on-polyethylene, cement-on-cement, or cement-on-polyethylene types. Surgeons that used metal-on-polyethylene spacers have reported that several methods can be used to recycle the hardware. In the first report on this topic, Hofmann et al.19) described a method for recycling previous femoral prosthesis using an autoclaving process, and their reimplantation using new polyethylene spacers. These authors reported excellent treatment outcomes and no case of reinfection among 26 cases over a mean follow-up period of 30 months. Thereafter several authors also reported excellent treatment outcomes for the same method.11172021) However, Kalore et al.22) used new femoral prostheses and a polyethylene insert due to concerns regarding the recycling of knee joint prostheses recommended for disposable use. In a study over a mean follow-up of 19 months in 16 cases, they reported no significant difference in infection control when femoral prostheses were autoclaved, but noted that the cost burden was appreciably greater when a new femoral prosthesis was used. Kim et al.13) recycled femoral and polyethylene prostheses after autoclaving, and reported one case of re-infection over a mean follow-up of 52.2 months in 25 cases. All patients achieved excellent treatment outcomes, with KS knee scores and FSs of 82 and 50 points, respectively.
Cement-on-cement and cement-on-polyethylene spacers provide the advantage of controlling and stemming infections by using antibiotic-loaded cement; however, they produce fragments, cannot be easily prepared in the operation room, and may prolong the operating time.232425) To resolve these shortcomings, customized spacers have been devised, but they are expensive. Also, the selection of appropriate antibiotics is limited.4101620)
In the present study, we used metal-on-cement spacers, which have not been previously described in literature, but which are cost-effective as compared with a new femoral component on polyethylene prosthesis. These metal-on-cement spacers are also advantageous in terms of preventing severe abrasion of the recycled polyethylene, because the mechanical strength of the recycled metal-on-polyethylene spacer is reduced during autoclaving.2627) In addition, as compared with the reimplantation of a polyethylene insert, metal-on-cement spacers allow a larger amount of antibiotics to be used. The surface area of cement mixed with antibiotics is also increased, and these characteristics probably afford more effective infection control. Furthermore, when compared with conventional cement spacers, metal-on-cement spacers require no specific technique when the cement is molded, since they can easily be molded by simple flexion and extension of the knee joint.
Unlike a polyethylene prosthesis, the range of motion is limited between the first and second stages of revision. In the present study, the mean range of motion was 72° prior to second-stage revision arthroplasty, and did not reach the 102.2° as reported by Kim et al.13) However, at final follow-up, the mean range of joint motion was 113° and mean HSS score was 86 points, which are similar to the results reported for polyethylene prostheses. Additionally, previous surgical sites and a medial parapatellar surgical approach were employed in all cases, and none of the patients required a rectus snip or tibial osteotomy for exposure, which indicates that excellent treatment outcomes were accomplished since no difficulty was encountered during second-stage revision arthroplasty due to joint contracture or quadriceps stiffness. Our technique might be used when the advisability of using recycled polyethylene is doubted after autoclaving, and when polyethylene cannot be recycled because of severe wear. In addition, it could also be useful in cases requiring a higher concentration of local antibiotics, such as in cases of MRSA infection.
Drainage was maintained for 3-5 days and splinting for a week, after the first revision stage. In previous studies, 28) maximal concentration of the antibiotics in the bone marrow was at 7 days after surgery. In our procedure, the maximal release of the antibiotics from the antibiotics mixed cement beads was on the very first day after surgery. Also, the bactericidal activity of the antibiotics in the bone marrow tissue was maintained for 6 weeks. If the drainage was removed within 2 days after surgery, it had an added advantage of maintaining the high concentration of the antibiotics within the joint. However, longer maintenance of the drainage for 3-5 days would be helpful in removal of the remaining debris, according to severity of the infection.
There are several limitations to this study. It was a retrospective and not a comparative study, and we had a small number of cases. The preoperative bacterial culture could be identified in only 9 out of the 20 cases, thus indicating that the diagnosis of infection for all cases can be difficult. Of the 13 patients transferred from the other hospital, most of them had already been administered antibiotics, resulting in a difficulty to identify the causative bacteria immediately.29) However, considering the clinical symptoms, laboratory tests, radiography, intraoperative findings, and histopathologic findings,30) we were able to diagnose the presence of an infection.
In summary, a two-stage revision arthroplasty involving autoclaving of the femoral prosthesis after removal from the infected knee joint prosthesis, followed by mobile prosthesis implantation by intraoperative molding of antibiotic-impregnated cement, provides excellent radiological and clinical outcomes. This novel technique offers a high surface area of antibiotic-impregnated cement as well as range of motion between first and second-stage revision surgery for the treatment of chronic infection after TKA. There is no additional cost to make the molded spacer. However, long term follow-up and observation are considered necessary.





 XML Download
XML Download