

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Synovial sarcoma is a malignant neoplasm comprising 5% to 10% of all other adult soft-tissue sarcomas (STS).1) Similar to most STS, synovial sarcoma has an aggressive and highly metastatic propensity. However, synovial sarcomas have distinct characteristics such as predilection for young adults and relatively slow growth compared with other STS. These unusual and diverse clinical features of synovial sarcomas frequently result in delayed diagnoses and unplanned excisions (UPEs).2,3)
When UPE is performed, it is widely accepted that re-excision is usually necessary to remove the possible residual tumor or to achieve adequate resection margins.4,5,6) Re-excision using wide margins that include normal surrounding tissues may cause significant morbidity and economic burden to patients.2,7) Thus, UPEs should be avoided.
Despite the relatively high incidence of UPEs of synovial sarcomas, few studies have focused on this issue.3,8,9) Identifying the characteristics of synovial sarcomas that were misdiagnosed and underwent UPEs would be beneficial in preventing an UPEs. In the present study, we aimed to assess the characteristics and outcomes of synovial sarcomas treated with UPEs.
METHODS
Patients' Clinical Characteristics
Patients who underwent surgery for 99 histologically proven synovial sarcomas of the extremities were included in this study. Of the 99 patients, we excluded 9 patients, including 6 with less than 2 years of follow-up and 3 with insufficient medical records; thus, 90 patients were eventually examined. All data were obtained retrospectively using medical records and radiographs after approval by the relevant Institutional Review Board.
Of the 90 patients, 34 were female and 56 were male. The mean age at diagnosis was 32.7 years (range, 5 to 80 years), including 20 patients (22%) younger than 20 years. The mean follow-up period was 6 years (range, 2 to 23 years). The lower limbs including the pelvis (n = 73, 81%) were more commonly involved than the upper limbs (n = 17, 19%). For analytical purposes, patients were divided into 2 groups: the planned excision (PE) group (n = 52, 58%), who received standard treatments for synovial sarcomas with no previous unplanned procedures, or the UPE group (n = 38, 42%), who underwent surgical treatments and in whom the possibility of sarcoma was not considered initially. Thirty-three patients (87%) of the UPE group were referred to our institutions after UPEs at other hospitals.
The medical records and magnetic resonance imaging (MRI) scans of patients in the UPE group, documented at the time of initial UPEs, were reviewed to identify the initially presumed diagnoses made at referring hospitals. We regarded pain, presence of swelling, tenderness and an enlarging mass as symptoms. Histopathology specimens obtained at the time of UPEs were examined by musculoskeletal pathologists of our institution. The verified tumor characteristics included the nature of tumor contents, size, anatomical location, depth, histological subtype, and histological grade. Histological grading was performed using the Federation Nationale des Centres de Lutte Contre le Cancer grading.10) For UPE, histological grading was performed by using specimens obtained at the time of UPEs or residual tumors detected during re-excisions. Out of 90 patients, MRI scans done prior to initial surgery were available for 73 patients (81%). Every patient in the UPE group had MRI scans prior to re-excision at our institute. Tumor size was defined by the maximal dimensions reported by pathological or MRI examinations. Tumor depth was graded as superficial or deep; tumors located exclusively above the superficial fascia without invasion of the fascia were defined as superficial.11)
Treatment Principles
Treatment principles comprised wide excision with or without adjuvant chemotherapy or radiotherapy. Surgery was performed to achieve wide margins by removing the cuff of normal tissues surrounding the tumors. Limb-sparing operations were primarily performed, if possible. All patients of the UPE group underwent re-excision to achieve wide resection margins. Adjuvant chemotherapy or radiotherapy was administered postoperatively when a higher risk of recurrence was believed to exist based on the clinical information, including histological grade, tumor size, presence of metastasis, and surgical margins. However, no prospectively determined criteria were used for patient selection. Adjuvant chemotherapy and radiation therapy were administered for 18 patients (47%) and 24 patients (63%), respectively. Disease-specific survival, metastasis-free survival, or local recurrence-free survival was assessed for documenting oncological outcomes. Specific deaths due to synovial sarcomas were documented as end points for disease-specific survival. Deaths by other causes were documented as censored. Local recurrence was defined as the first recurrence of disease at the primary tumor site after resection.
Statistical Analysis
Overall survival, metastasis-free survival, and local recurrence-free survival were estimated using the Kaplan-Meier estimator. Survival curves for both groups were evaluated using the log-rank testing for univariate factors and Cox's stepwise regression for multivariate factors. Relative risks were calculated using a proportional-hazards model. Comparison of the categorical variables between the PE and UPE groups was performed using the Fisher exact test and Pearson chi-square test. Statistical analyses were performed using the PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Comparison of Clinical Characteristics between the PE and UPE Groups
Among the clinical characteristics, the duration of symptoms before diagnosis was significantly longer in the PE group than that in the UPE group (p = 0.023) (Table 1). UPEs were more often performed for small (< 5 cm) and superficially located lesions (p = 0.001 and p = 0.049, respectively). Of the 20 upper-limb lesions, UPEs were performed for 12 (60%), compared to 26 (36%) of the 73 lesions located in the lower limb (p = 0.037). Initial metastases were detected in 13 patients (14%). The proportion of patients presenting with metastasis at diagnosis was not significantly different between the PE group (10 patients, 19%) and UPE group (3 patients, 8%; p = 0.112).
Patterns of Misdiagnosis
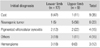
MRI scans prior to initial UPEs were available for 26 patients (68%) in the UPE group. Gadolinium enhancement was used in only 8% of cases in the UPE group compared to 96% in the PE group (p < 0.01). When the initial MRI reports of the 26 UPE patients were analyzed, a misdiagnosis pattern was observed with regard to tumor location (Table 2). In the lower limbs, almost half (8/17, 47%) of synovial sarcomas were misdiagnosed as cystic masses (popliteal cysts or meniscal cysts) around the knee (Fig. 1), whereas synovial sarcomas were most commonly misdiagnosed as neurogenic tumors (5/9, 56%) in the upper limbs (Fig. 2).
Oncological Outcomes and Prognostic Factors
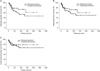
At the time of analysis, 26 patients (33%) had died of causes associated with synovial sarcoma and 2 patients had died of other causes. Five-year oncological outcomes, including disease-specific survival (64% vs. 73%, p = 0.159), metastasis-free survival (65% vs. 73%, p = 0.444), or local recurrence-free survival (77% vs. 79%, p = 0.335), were not significantly different between the PE and UPE groups, respectively (Fig. 3).
UPE Treatments
The number of UPEs prior to definitive re-excision ranged from 1 to 4 (mean, 1.36). Patients with a multiple number of UPEs (n = 8) had significantly higher rates of local recurrence than patients (n = 30) with single-excision operations (p = 0.012). The median interval between UPEs to re-excisions was 6 weeks (range, 1 to 132 weeks). Patients with intervals longer than 4 weeks (n = 19) to re-excision had significantly higher rates of local recurrence than patients with intervals shorter than 4 weeks (n = 19) to re-excision (p = 0.038). Of the 38 patients in the UPE group, residual tumors were detected in re-excised specimens in 31 patients (82%), including 29 with macroscopic residual tumors. However, the local recurrence rate did not significantly differ between the patients with residual tumors and patients without residual tumors (19% vs. 14%, p = 0.617).
DISCUSSION
Synovial sarcoma is often managed erroneously by UPEs because they are often misdiagnosed as benign masses. Synovial sarcomas are misdiagnosed because they occasionally shows atypical STS characteristics such as early onset in young adults and slow growth. There have been no reports documenting misinterpretations of imaging studies or clinical outcomes of synovial sarcomas inadequately treated with UPE. Our study compared oncological outcomes of synovial sarcomas following UPE with those treated by standard procedures.
Synovial sarcomas are frequently diagnosed late or excised inadequately because of their slow growth rates and apparently harmless symptoms.7,12) A study of the presentations of 33 synovial sarcoma patients found that only half of synovial sarcoma patients had typical STS symptoms and the mean delay until correct diagnosis was 50 weeks.7) The average duration of symptoms ranged from 2 to 4 years, and up to 20-year histories have been reported.1) Indeed, the duration of symptoms until diagnosis was significantly longer in the UPE group than in the PE group in our study. Moreover, synovial sarcomas are reportedly misdiagnosed most frequently as benign lesions by MRI, whereas only one-third of synovial sarcomas actually show benign characteristics.9,13) Synovial sarcomas present as well-defined masses with smooth, round, or gently lobulated margins and are usually localized rather than invading surrounding structures.14)
The review of MRI scans of UPE cases revealed a clear trend for anatomical location and tumor size. Our data showed that common misdiagnoses differed according to tumor location; synovial sarcomas were most commonly mistaken for neurogenic tumors in the upper limbs (56%) and cysts in the lower limbs (47%). Relatively small-sized synovial sarcomas tended to be more homogenous on MRI scans, making it difficult to diagnose them differentially from neurogenic tumors in the upper limbs.8) On the other hand, relatively large-sized synovial sarcomas were usually heterogeneous with cystic or necrotic components, making them likely to be diagnosed as cystic masses in the lower limbs.14) Contrast-enhanced MRI has been reported to be effective in differentiating a STS from a benign soft tissue tumor.8,9,14) In accordance with previous reports, most erroneous diagnoses were made using MRI scans without contrast enhancement.
The incidence of the detection of residual tumors at re-excisions was high (82%) in the current study cohort compared to reports studying other STS from 23.6% to 45%.4,5,6,15) However, the local control rates did not differ. According to these results, synovial sarcoma has tendency to show residual lesion after UPE than other kind of STS. Despite the incidence of residual tumors being 82%, the authors reported a 5-year local recurrence-free survival of 79%.
Oncological outcomes were similar between the PE and UPE groups in our study despite the potential negative effects of the complications of UPEs on patient outcome. The comparable oncological outcomes observed in both the UPE and PE groups could be attributed to the fact that known prognostic factors, such as small in tumor size and superficial in location, were more favorable in the UPE group.16,17) In the UPE group, delayed re-excisions and repeated UPEs were associated with poor local control in contrast to a previous report.4) Therefore, it is advisable for the patients to undergo re-excision as soon as possible.
We studied a relatively small patient cohort because cases of synovial sarcomas are rare. However, our report is unique because we studied the largest series of synovial sarcoma cases that had undergone UPEs, to date. Although, this study was conducted in 2 separate tertiary-referral sarcoma centers, the same principles of treatment were applied to all patients. Immediate re-excisions were performed for all the UPE patients and aggressive adjuvant treatment was recommended for all patients with residual tumors.
In conclusion, synovial sarcomas treated with UPEs had distinct characteristics, including small lesion sizes, superficial location and high risk of residual lesion. UPE was done more frequently in the patient with MRI without enhancement. Synovial sarcomas were most commonly misdiagnosed as neurogenic tumors in the upper extremities or as cystic masses in the lower extremities. Contrast-enhanced MRI is effective in differentiating a malignant mass from a benign mass in synovial sarcoma diagnosis. These findings are important for developing diagnostic and therapeutic strategies for synovial sarcoma.



 XML Download
XML Download