

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hip fractures are relatively common in the elderly and are fast becoming a major public health issue in this population group.1) Current estimates are that over 70,000 hip fractures occur every year at a cost of over £2 billion.1) Neck of femur (NOF) fractures may be intracapsular or extracapsular, displaced or undisplaced and these important distinctions help guide the management of the injury. Any type of intracapsular NOF can cause a disruption in the blood supply to the femoral head. This coupled with the presence of little cancellous bone in the head and neck means these fractures are often complicated by non-union and avascular necrosis (AVN).
Treatment of this injury is usually surgical in nature in the form of arthroplasty or fracture fixation; however, fixation has been associated with significant fracture healing complications. In his meta-analysis of 106 studies of displaced NOF, Lu-Yao et al.2) reported a non-union rate of up to 20%-40% and AVN rates of up to 16% within a 95% confidence interval for displaced fractures. Still surgical fixation remains an option which allows the retaining of the native femoral head as the alternative would be some form of joint replacement surgery, especially in younger patients.
Various fixation methods have been described in the literature over the years. In their recent Cochrane review of internal fixation implants for intracapsular hip fractures in adults, Parker and Stockton,3) identified 18 different implants from 30 studies and still were unable to show superiority of one over the other from the data reviewed. Traditionally, the sliding hip screw (SHS) and the multiple cancellous screws (MCS) have been the most commonly used fixation methods and both have produced good results in the literature.
The Targon FN (B-Braun AG, Melsungen, Germany) implant was developed in 2007 to treat NOF fractures (Fig. 1). It is a locking plate system with telescoping sliding screws, combining the best features of the MCS and the SHS fixation methods. Early results from the design centre have shown good results. Parker and Stedtfeld,4) reviewed 83 patients treated with this implant and with a minimum 1-year follow-up. It reported a 3% and 7% non-union rate for undisplaced and displaced fracture groups, respectively. This suggests a superior outcome to results for other fracture fixation methods in the literature.
This system was introduced in this institution in 2008 and is now the favoured method of fixation for these kinds of fractures. Prior to this, the MCS and SHS were the fixation methods of choice. The real test for this new fixation device remains the replication of similar outstanding results in 'non-expert' hands outside of the design centres. Hence the aim of this study was to report our experience of the use of this device in the treatment of intracapsular NOF. As far as the authors know, it will be the largest study to look at the Targon FN implant outside of its design centre.
METHODS
Case notes and X-rays of consecutive patients, who had Targon FN fixation for intracapsular NOF fractures between 2008 and 2011 at Queen Elizabeth Hospital, were identified and reviewed for this study. As this was a retrospective study, they were no specific inclusion and exclusion criteria; however, most of these were mainly patients those with undisplaced fractures and displaced fractures in the younger age group of patients. These groups of patients are usually followed up in fracture clinic according to longstanding local departmental practices due to the risk subsequent AVN and also depending on the age of the patient at presentation. Each patient had a minimum follow-up of 24 months. Patients unable to attend clinic for any reason were assessed over the phone with regards to general function and level of mobility. If it is found to be significantly symptomatic, arrangements were made for these patients to be assessed clinically and radiologically. The study was carried out in accordance with local Departmental of Clinical Audit approval.
The implant system consists of a short femoral locking side plate mounted on an external jig and with the potential for up to 46.5 mm telescopic sliding screws (Telescrews) going into the femoral neck and head that allows for fracture collapse. The sliding for the collapse occurs within these Telescrews and with the screw locking onto the plate, no protrusion of screw into the lateral (LAT) soft tissue can occur. The plate is fixed to the femur using two 4.5 mm cortical screws. The implant is suitable for use in displaced and undisplaced NOF fractures.
Surgical Technique
All operations were carried out by all grades of surgeons independently and under supervision as needed. The surgical technique as described by the manufacturers and similar to that employed by Parker5) in his study was used. The patient is positioned on the fracture table similar with a SHS fixation. Undisplaced fractures were fixed in situ (Fig. 2). Displaced fractures were reduced by gentle longitudinal traction and internal rotation to the best position as seen on both the anteroposterior (AP) and LAT views (Fig. 3). Not more than one attempt at reduction was encouraged. A 5-10 cm LAT incision is made just distal to the greater trochanter and soft tissue dissection is carried out down to the LAT cortex of the proximal femur. The Targon plate, fixed to an alignment jig is positioned centrally on the LAT cortex so as to allow a guide wire to be passed through the centre of the femoral neck and into the femoral head on both AP and LAT views stopping just before or within the subchrondral bone. The other guide wires are now passed in similar fashion through the plate and jig for the Telescrews, the final number used (at least 3) was at the discretion of the operating surgeon. The length of the guide wires is then measured, drilled and each Telescrew is inserted in turn, locking onto the side plate. These Telescrews can be extended further by up to 10 mm to adjust their final position right up close to the subchrondral bone. The plate is further fixed distally by two distal screws inserted through the jig. The wound is then closed in layers. Mobilisation can be commenced immediately or in phases as prescribed by the operating surgeon for the particular patient.
RESULTS
Fifty-one consecutive patients were as having had a Targon FN fixation for intracapsular NOF fractures. Six of these were excluded from the study as they died within 6 months of the operation of unrelated causes and 2 had moved out of the area and could not be contacted. Hence, 43 patients completed the minimum follow-up period of 24 months (range, 24 to 47 months) and were reviewed for this study. They were 33 females and 10 males with a mean age of 66 years (range, 24 to 94 years). They were 31 (72%) undisplaced and 12 (28%) displaced NOF type fractures. Twenty-nine were admitted from their own homes while 14 came from a cared setting. Mean duration for surgery was 67 minutes (range, 39 to 100 minutes). Average time to study for all fractures was 27.4 hours. Three Telescrews were used for fixation in all cases in the study. Twentynine procedures (67%) were carried out by consultants or with scrubbed supervision while 14 (33%) were carried out independently by trainees or staff grades.
An overall non-union rate of 2% was observed from 1 case of non-union occurring in the displaced NOF group (8%). No such case was found in the undisplaced NOF group (0%). This non-union occurred in a 25-year-old patient with social problems and compliance issues. After 5 months, check X-rays showed the fracture had displaced though the patient denied any new trauma. After consultation with a tertiary referral centre, the decision was made to convert to a total hip replacement (THR). The patient has no further complications since.
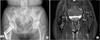
Three cases of AVN were also observed in this study giving an overall AVN rate of 7%. Two cases (6%) occurred in undisplaced group while 1 (8%) occurred in the displaced fracture group (Table 1). The first case from the undisplaced group was noted after 17 months after presenting with pain in the hip join and radiographs confirmed the diagnosis. The next case was from the displaced group of fractures and was observed after 20 months. Three Telescrews were used for fixation in this case. Both of these cases were later converted to a THR and are both doing well at latest follow-up. The last case was from the undisplaced fracture group, presenting after 20 months with hip pain and the diagnosis was confirmed with a magnetic resonance imaging (MRI) scan (Fig. 4). This patient was also converted to a THR. This gives an overall reoperation rate of 7% for this implant in this study.
No postoperative wound healing complications were observed in all patients during the period covered by this study. Postoperative mobilisation was as prescribed by the operating surgeon though with an emphasis on full weight-bearing mobilisation when clinically appropriate. Parker5) advised a period of partial weight-bearing mobilisation for up to 6 weeks for younger patients with a displaced fracture in his study. Also at their latest follow-up and/or communication, no patient reported a significant change or loss of mobility compared to their premorbid status.
DISCUSSION
Surgical fixation of NOF fractures is based on the need to maintain either the stable configuration of the undisplaced fracture or the position after reduction of the displaced fracture, so as to allow for fracture union.3) The fixation should provide a stable bone and implant structure that is strong enough to carry the weight-bearing load. MCS fixation can be carried out with minimally invasive techniques hence less soft tissue trauma. It also improves torsional strength and preserves femoral head blood supply more than the SHS by retaining more viable cancellous bone due to the small diameter of the screws inserted, potentially reducing non-union and AVN rates. Madsen et al.6) in their randomized control trial comparing SHS and MCS showed a 2-year cumulated union rate of 64% for the SHS and 84% in the MCS group.
Early fixation failure with the use of MCS can occur in the presence of a comminuted LAT cortex, particularly in osteoporotic bone. Fixation failure can also occur with the bending and vertical shear loading forces as seen in weight-bearing. The SHS is a plate with a sliding screw rather than a rigid fixed angle neck screw. The SHS with its larger screw diameter achieves better biomechanical strength and fixation particularly in osteoporotic bone. In a cadaveric model, Linke et al.7) showed a SHS system had a better fixation strength and stability, under cyclic physiological loading (weight-bearing), in osteoporotic bone than the MCS. It minimises the risk of subtrochanteric fractures due to the stress riser effect which is seen in MCS fixation. The sliding nature of the SHS allows for both compression and impaction of the fracture to promote healing. SHS, however, requires a larger surgical exposure and the use of a single large screw removes more cancellous bone which can affect femoral head blood supply. There is also an increased risk of rotational misalignment of the femoral head and neck during implant insertion.
Hence, the ideal fixation device should then combine the best qualities of both SHS and MCS designs into one improved implant with even better biomechanical properties. Parker5) identified these features which have been incorporated into the development of the Targon FN plate and screw system. Some of these features are outlined in Table 2.
Brandt and Verdonschot8) in their cadaveric biochemical analysis of the SHS, MCS, and the Targon FN showed the load to failure was significantly higher for this new implant than for the SHS, which was the same as for the MCS. They concluded that the Targon FN implant showed an increase mechanical strength of reconstruction in displaced intracapsular NOF fractures.
The results from this study compares favourably with those from the Targon FN design centre and also with the literature. From their design centre, Parker and Stedtfeld4) showed an overall non-union rate of 9.6% compared to a 2% rate in this study. This breaks down to 0% and 8% non-union rate in both the undisplaced and displaced fracture groups, respectively in our study compared to 3% and 15%, respectively in the design centre study. These figures are comparable or better than those from the review of literature that reports a rate of 6% (Conn and Parker9)) and 33% (Lu-Yao et al.2)) for undisplaced and displaced fractures, respectively.
With regards to AVN complications, the Parker and Stedtfeld4) study showed a rate of 3% for undisplaced and 7% for displaced fracture types while this study showed a rate of 6% and 8%, respectively. Both results again compare favourably to the rates found in the studies of Conn and Parker9) of 4% and that of Lu-Yao et al.2) of 16% for undisplaced and displaced fracture types, respectively. While the Targon FN provides for 4 screw fixation, the above results were obtained using 3 Telescrews which is acceptable and also described in other studies from the design centre.5,10) The use of 3 screws was purely incidental and could be ascribed to surgeons choice and/or an unconscious view on cost implications. It would be interesting to see the effect, if any, of using 4 Telescrews on these fracture healing complications. It can be argued that the use of 4 Telescrews may give a more secure fixation particularly in the displaced fracture group, which can potentially reduce the non-union rate. Conversely, with more metalwork within the femoral head, potentially AVN could be possible.
Korver et al.11) also reported their clinical experience of 16 patients with this implant. They noted 2 patients (13%) with non-union requiring a reoperation. It also highlighted some potential technical difficulties including guidewire placement, lack of a tactile feedback and risk of penetrating the subchrondral plate. In the most recent update of their patient cohort, Parker et al.10) with 320 consecutive patients, now reports a non-union and AVN rate of 2.7% and 4.5% from 112 undisplaced fracture group. From 208 displaced fractures, it reported a non-union and AVN rate of 15.4% and 11.1%, respectively.
The use of MRI for the diagnosis of AVN in this study highlights a significant advantage of the Targon FN implant over other forms of fixation. This new implant is made of titanium which makes it compatible with use in the MRI scanner, hence eliminating the compatibility problems experienced with stainless steel composition of the more traditional MCS and SHS fixation methods. This can give the surgeon a significantly improved diagnostic accuracy in the investigation of fracture healing complications.
The results of this study backs up the excellent results from the design centre for the use of this implant in the treatment of NOF fractures and also from the other limited studies available. More significantly for any new implant, it confirms that these good results can be reproduced outside of the design centre and in the hands of non-specialist surgeons, including trainees, in a routine district general hospital setting. The limitations of this study include its retrospective nature, the small number of patients and the lack of a control group and randomisation of patients. The minimum 2-year follow-up period for this study improved the observational strength of the study compared to other studies in picking up fracture healing complications which can take up to 2-3 years to develop. Still, there is the need for more robust studies or clinical trials to further evaluate this device and in comparison with the other traditional fixation methods.
With projected changes in the population demographics set to produce an ever increasingly ageing population, the intracapsular NOF threatens to become a bigger headache than what it is today. With this study and others, the Targon FN device shows a strong potential in reducing fracture healing complications in the treatment of these injuries and thus, reduce the burden of revision surgery which is not always successful. As such, future research in the form of more robust studies with larger numbers and longer follow-up are needed to further evaluate this device. Also, comparison studies with the other traditional fixation methods.





 XML Download
XML Download