

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The reported incidence rate of septic arthritis following anterior cruciate ligament (ACL) reconstruction ranges from 0.4%-1.7%1) with the majority of infections caused by Staphylococcus aureus and S. epidermidis.1) Mycobacterium infections following ACL reconstructions are rare, with only 9 reported cases in the literature.2,3) To our knowledge, there are no previous reports citing Mycobacterium abscessus as the culprit pathogen.
M. abscessus comes from the family of rapidlygrowing Mycobacterium (RGM), which have been implicated in prosthetic joint infections postoperatively. Such infections are some of the most challenging to treat due to their high pathogenicity and resistance to chemotherapy. The bacterium is typically found in soil, sewage and natural water sources, and has been associated with nosocomial surgical site infections, as well as lung and soft tissue infections.4)
We describe a patient with a M. abscessus infection following ACL reconstruction. The purpose is to describe the clinical features and course of such an infection following ACL reconstruction as well as other key learning points.
CASE REPORT
We report a case of a healthy 22-year-old man who underwent an arthroscopic right ACL reconstruction with hamstring grafts in January 2010, 6 months after his initial injury. There were no associated injuries. The graft was fixed with an Endobutton (Smith & Nephew, Andover, MA, USA) for the femoral side, and a Biosure bioabsorbable screw (Smith & Nephew) and metal staples (Smith & Nephew) for the tibial side. After an initial uneventful postoperative recovery, he presented 7 weeks after surgery with right knee swelling associated with fever and chills. On examination, there was dehiscence of the tibial tunnel wound with hemoserous discharge. The range of motion of the right knee was 5° to 100° and was limited by pain. The C-reactive protein, erythrocyte sedimentation rate, and total white cell count were 139, 71, and 7.3, respectively. The right knee aspiration performed revealed turbid fluid, and bacterial cultures yielded no bacterial growth.
He was offered, but refused, arthroscopic debridement of the right knee, and was given oral antibiotics with instructions to follow-up at the outpatient clinic. There was no resolution of his wound discharge, and the patient subsequently consented to an arthroscopic washout of his right knee, synovectomy, and debridement of the right tibial wound 3 months after his initial ACL reconstruction. Intraoperatively, there was florid synovitis but the ACL graft was noted to be intact and healthy. There was no frank pus noted from the right tibial wound and the wound was debrided. The bioabsorbable screw and staples were left in situ.
The knee fluid was incubated at 35℃, 5% carbon dioxide levels on blood agar for five days. It revealed scanty growth of a non-tuberculous RGM. The mycobacterium detection DNA Accuprobe identification was positive and the organism was confirmed to be M. abscessus. Susceptibility testing using a broth microdilution method confirmed that the organism was sensitive to amikacin, clarithromycin, and linezolid.
Postoperatively, the patient was given 2 weeks of intravenous (IV) amikacin and concurrently started on one week of IV cefoxitin and clarithromycin. There was a gradual decline in the laboratory markers of infection (Creactive protein and erythrocyte sedimentation rate). He was subsequently treated with 4 months of oral clarithromycin and bactrim. Postoperatively, the wound showed progressive healing, with no further discharge noted during subsequent outpatient consultations. He was lost to follow-up 6 months after the arthroscopic washout and 9 months after his initial ACL reconstruction.
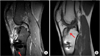
Two years later, he presented to our outpatient clinic with right knee pain associated with discharge from the knee wound for the past six months. There was no associated fever. There was a chronic sinus located over the anteromedial aspect of the right knee with seropurulent discharge, giving the appearance of a chronic granuloma. There was otherwise no collections seen and the ACL graft appeared intact (Figs. 1 and 2).
The patient subsequently underwent arthroscopic washout and removal of the screws and staples of the right tibia. Intraoperatively, he was noted to have a chronic sinus tract over the staples and tibial tunnel site. The screw was loose and fragmented, with surrounding sloughy tissue seen. The ACL was noted to be lax on arthroscopy (Fig. 3).
In view of his previous history of M. abscessus infection, the patient was started on IV amikacin, cefoxitin, and oral clarithromycin. The initial bacterial cultures showed moderate growth of S. aureus. However, subsequent delayed cultures at 6 weeks grew M. abcessus. The histology demonstrated inflamed granulation tissue with no granulomas seen. He received 14 days of IV amikacin, IV cefoxitin, and oral clarithromycin for the duration of his hospitalization. He was discharged on postoperative day 17 with 6 weeks of oral clarithromycin and 2 weeks of oral cloxacillin.
The patient was successfully contacted for a clinical review 14 months after the second arthroscopic washout and implant removal from his right knee. He reported no further symptoms of infection in his right knee since the second arthroscopic washout and had regained full premorbid function of his right knee. On examination, the wounds had since healed, the knee was not warm, effused, or tender and there was full range of motion of the right knee. However, he demonstrated a positive Lachman's test (Fig. 4).
DISCUSSION
After its separation from the M. chelonae group in 1992, M. abscessus was recognized as the culprit pathogen for many human infections, including skin and soft tissue infections, surgical site infections, respiratory infections, and disseminated infections in immunocompromised individuals.
Infections caused by M. abscessus are notoriously difficult to treat because the bacteria is intrinsically resistant to most conventional anti-tuberculous drugs. Reasons for this resistance include the slow growth of the bacteria, the presence of a waxy impermeable cell wall, which serves as both a physical (by size exclusion) and a chemical (hydrophobic) barrier, various drug export systems, and genetic polymorphism of targeted genes.4) M. abscessus possesses the ability to form smooth biofilms. Hence, retention of the implants can possibly lead to a failure to achieve a microbiological cure and re-infection, especially since M. abscessus is notoriously resistant to most antibiotic regimes.
There are published case reports of M. abscessus bacteremia associated with infected indwelling vascular catheters. A case series by Chang et al.5) involving 12 patients with RGM bacteremia demonstrated that the rate of relapsing bacteremia was significantly higher in patients with delayed catheter removal compared to patients with timely catheter removal. In our case report, the patient's implants were initially left in situ, as it was deemed too premature to remove the implants because the graft had not yet integrated. However, leaving the implants in place may result in the persistence of infection, as shown in the vascular catheter case series. Thus, the first learning point is the need for full removal of implants in M. abscessus infections for source control in persistent, recurrent infections.
The literature demonstrates a lack of consensus for the treatment of septic arthritis following ACL reconstruction. Generally, the treatment involves either arthroscopic or open debridement with or without ACL graft retention followed by antibiotic treatment. McAllister et al.6) reported an average of 2.75 procedures (range, 2 to 4 procedures) required after the diagnosis to eradicate the infection and restore knee motion. The scar formation resulting from repeated invasive procedures to the involved knee joint can lead to capsular contraction, thus significantly limiting joint motion and affecting the patient's functional outcome.
A recent case report describing a M. wolinskyi infection post-total knee arthroplasty emphasizes the lack of a standardized treatment protocol in infections caused by RGM. In the case report, the authors described the successful eradication of the infection after prolonged targeted antibiotic therapy and surgical debridement without removal of the prosthesis.7) This suggests that the decision as to retain or remove the implant should be taken on a case-by-case basis.
There is limited literature on the incidence and management of culture-negative septic arthritis following ACL reconstruction. However, there are publications delineating the incidence of culture-negative prosthetic joint infections. Berbari et al.8) described 60 cases (7%) of culture-negative prosthetic joint infections out of 897 patients with prosthetic joint infections over a 9-year period. These 60 patients were noted to have a sinus tract or purulence communicating with the prosthesis and/or features of acute inflammation on histology. The possible reasons for culture-negative infections are prior antimicrobial therapy, infection with fastidious organisms or unusual organisms such as fungi or mycobacterium, and biofilm formation. Our patient had a similar presentation and his initial cultures did not yield any bacterial growth. Hence, the second important learning point is that in patients presenting with chronic discharging sinuses over the previous surgical site with negative cultures, infection with RGMs such as M. abscessus should be considered.
There have been case reports of coinfections as well as secondary infections of prosthetic joints. The implicated organisms include Listeria monocytogenes with S. aureus9) and Candida albicans with Methicillin-resistant S. aureus.10) Hence, a third learning point is the need to consider the possibility of a coinfection or superinfection whenever there is an atypical organism involved, such as M. abscessus. The presence of a secondary or coinfection in post-ACL reconstruction septic arthritis is clinically relevant, as it significantly affects the choice of antimicrobial therapy. It should also be considered in cases of infection which do not respond to the antimicrobial regime tailored to the initially identified organism. In our case, the chronicity of the discharge and low grade nature of the infection suggested an atypical infection. However, the presence of a purulent component to the discharge suggested an element of coinfection with a Staphyloccal species.
In our patient, the biosure bioabsorbable screw used was made of poly-L-lactic acid and hydroxyapatite. Polylactic acid implants are thought to be less likely to cause local inflammatory and foreign body reactions as compared to similar implants manufactured using polyglycolic acid, due to the long degradation time of polylactic acid.3) Despite this, abscess cavities in conjunction with the l tunnel have been reported, with negative gram stains and cultures.3) During the second debridement of our patient, the screw in the tibial tunnel was noted to be loose and fragmented, suggesting that the local inflammatory response from osteolysis associated with the use of a polylactic implant may provide a suitable environment for infection to occur.
Our case report has demonstrated that atypical organisms, such as M. abscessus, should be considered whenever bacterial cultures are negative in chronic lowgrade infections. The possibility of coinfections and superinfections in such cases should also be considered. The case also suggests that removal of orthopedic implants may be necessary for the complete eradication of this pathogen.



 XML Download
XML Download