

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ambulatory surgeries account for an increasing share of all surgical procedures. More than 60% of all surgeries in the US and Europe are performed in ambulatory settings, and in particular, hand and wrist surgeries have shown an increasing trend.1,2,3) Advances in less invasive surgical techniques, the use of short-acting general anesthetics and the cost-effectiveness of ambulatory surgeries have contributed to an increasing number of surgeries performed in ambulatory settings.4)
The perioperative care for a patient's quality of life is an important concern in an ambulatory surgery.5) However, many patients undergoing ambulatory surgery under general anesthesia experience unacceptable levels of nausea and vomiting (N/V) after surgery.6,7) Although ambulatory patients are less likely to experience postoperative N/V than inpatients, this could be partly explained by an under-recognition of postdischarge N/V because ambulatory patients are not under direct medical supervision after their discharge.8) Most of hand surgeries can be performed under regional anesthesia, thus they are not typically thought to result in a high incidence of postoperative N/V.9,10) However, considerable parts of hand surgeries are still being performed under general anesthesia and a study reported up to 32% incidence of postoperative N/V after ambulatory hand surgeries under general anesthesia.11)
A number of studies have addressed postoperative N/V in areas such as gynecological,9) abdominal,10) ears, nose and throat,12) or arthroplastic surgery of the knee.13) However, incidences of those events are known to be influenced by the type of surgical procedure,6,14) as the surgical location, such as abdominal surgery or a head and neck (near the ear) surgery can affect N/V levels. Also patients undergoing lower extremity surgeries that require admission may get a better treatment of their N/V. Furthermore, few studies have comprehensively evaluated factors associated with postoperative N/V in ambulatory hand surgeries. Therefore, we investigated factors associated with postoperative N/V in patients undergoing an ambulatory hand surgery under general anesthesia and determined whether patients' satisfaction with this setting is associated with postoperative N/V levels.
METHODS
Subjects
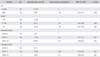
The Institutional Review Board at Seoul National University Bundang Hospital approved this study. Inclusion criteria for an enrollment in this study were: (1) patients older than 16 years who were scheduled to undergo an elective hand surgery under general anesthesia, which involved surgeries for forearm fractures, tendon, and nerve as well as elbow surgeries and (2) the preoperative agreement to participate in this study. We excluded patients who underwent a surgery with regional anesthesia, patients with medical comorbidities preventing an ambulatory hand surgery, regular use of narcotics and mental illness or disability. Thus, we prospectively recruited a total of 200 consecutive outpatients. Of these 200 patients were 59 male and 141 female and their ages ranged from 16 to 77 years (average age, 50.3 ± 16.1 years) (Table 1).
Evaluation of Factors Associated with Postoperative N/V
Based on previous studies considering various predictors of postoperative N/V,2,12,14,15) we considered several potential predictors: age, sex, the body mass index (kg/m2), smoking behavior, history of postoperative N/V after previous anesthesia or motion sickness, preoperative anxiety level and duration of anesthesia. The type of surgery (bone or soft tissue surgery) was not considered as a predictor of N/V, although this could be related with postoperative pain.
A single research assistant asked the patients during preoperative visits regarding their smoking behavior, history of postoperative N/V experiences from previous surgeries or motion sickness (yes or no) and preoperative anxiety levels. The smoking history was evaluated based on the smoking status (current or former) versus never smoking. Preoperative anxiety levels were assessed using the Amsterdam Preoperative Anxiety and Information Scale (APAIS),16) which was proven to be a valid, reliable and easily applicable instrument for assessing the level of patients' preoperative anxiety.17)
All patients received 650 mg acetaminophen three times a day as their postoperative pain medication for seven days prior to the surgery. Each patient visited the outpatient clinic on the day after the surgery for wound dressing and was asked by the same research assistant about their N/V and pain levels during the first 24 hours after surgery using a visual analogue scale (VAS) ruler. A VAS was used ranging from 'not nauseated' (0) to 'extremely nauseated or vomiting' (100) to measure N/V. This scale was applied in previous studies.18,19) A scale was used ranging from 'no pain' (0) to 'extreme pain' (100) to measure the postoperative pain during the first 24 hours. The overall satisfaction with the ambulatory hand surgery setting was evaluated by asking the patients of their willingness to undergo the same surgery under the same ambulatory setting without being admitted for further care for perioperative discomforts (yes or no style). In addition, we documented any complication associated with the ambulatory anesthesia.
Analyses
We set the number of events per variable in the linear regression analysis to 20 to avoid a major bias problem. As a result, a total of 160 patients were required to evaluate the 8 independent variables as potential predictors of postoperative N/V. For the univariate analysis, we compared continuous variables through the t-test or ANOVA and evaluated the relationships between the continuous variables by using Pearson correlation coefficient. Here, the main outcomes or response variables were the levels of postoperative N/V. We included those independent variables that were significant at p < 0.1 in the multivariate regression model. We conducted a multivariate linear regression analysis with stepwise variable selection to identify the independent predictors of postoperative N/V.
We also conducted a logistic regression analysis to examine the relationships between the patients' postoperative N/V and their overall satisfaction with the ambulatory hand surgery setting. Multivariate logistic regression analyses were performed using satisfaction as the dependent variable and the independent variables included sex, age, postoperative pain and N/V. Here, the statistical significance was indicated by p < 0.05.
RESULTS
The postoperative N/V score was higher in patients who were nonsmokers and had a history of motion sickness (p = 0.04 and p = 0.01, respectively). In addition, postoperative N/V level had a significant positive correlation with the preoperative anxiety level (r = 0.301, p = 0.017) and with the duration of surgery (r = 0.265, p = 0.020). According to the multivariate analysis, postoperative N/V levels (VAS) had significant positive relationships with motion sickness, preoperative anxiety and non-smoking and a model including these factors accounted for 21% variability of the postoperative N/V (R2 = 0.21) (Table 2).
Of the 200 patients, 11% were not satisfied with the ambulatory setting and refused to undergo the same surgery with the same setting. This dissatisfaction with ambulatory hand surgery was associated with moderate (VAS 4-7: odds radio [OR], 0.28; 95% confidence interval [CI], 0.09 to 0.88) and high (VAS 8-10: OR, 0.03; 95% CI, 0.01 to 0.30) levels of postoperative N/V compared with mild levels of postoperative N/V and high postoperative pain (VAS 9-10: OR, 0.11; 95% CI, 0.03 to 0.43) compared with mild levels of postoperative pain (Table 3).
DISCUSSION
For patients undergoing an ambulatory surgery, a sufficient postoperative management of N/V is an essential part of perioperative care because the surgery entails those discomforts and thus reduces patients' satisfaction with it.20,21) However, these complications have not been thoroughly assessed previously in hand surgeries which are commonly performed in an outpatient setting. This study demonstrates that postoperative N/V was associated with a non-smoking history, a history of motion sickness and a high level of preoperative anxiety in patients undergoing an ambulatory hand surgery under general anesthesia. This study also confirms independent of postoperative pain that postoperative N/V is associated with patients' dissatisfaction with the ambulatory hand surgery setting. Specifically, the dissatisfaction with an ambulatory hand surgery was associated with moderate as well as high levels of postoperative N/V, while the dissatisfaction was associated with a high level of postoperative pain only. This suggests that patients who undergo an ambulatory hand surgery may regard a low to moderate level of postoperative pain as an unavoidable outcome accompanying the surgery, but may have a lower threshold for postoperative N/V compared with postoperative pain.
In this study, patients without history of motion sickness or were smokers experienced a lower level of postoperative N/V than those with a history of motion sickness or were nonsmokers. This is generally concurrent with the findings of previous studies.7,15) Patients with a history of motion sickness are reported to have a low threshold for nausea or vomiting,22) and to have a well-developed reflex arc for vomiting.23) Nonsmokers also have been identified as being at higher risk of developing postoperative N/V than smokers.24) The chemicals in cigarette smoke were known to increase the metabolism of several drugs used in anesthesia, which results in a decreased incidence of postoperative N/V.25)
Our study suggests that preoperative anxiety is associated with an increased postoperative N/V in patients, although the literatures considering preoperative anxiety as a predictor of postoperative N/V produced conflicting results.18,22,26) Although little evidence was available for a relationship between anxiety and nausea after anesthesia, a high catecholamine release in patients with anxiety has been suggested to be a contributing factor for the development of emesis.22,23,27) An excessive air swallowing in anxious patients, which can increase the gastric volume may also be related to the increased incidence of postoperative emesis.22) Van den Bosch et al.26) reported that high levels of preoperative anxiety are associated with the occurrence of postoperative N/V, but that the association is weak and routine preoperative measurement of anxiety may not be warranted. Further studies are necessary to evaluate whether attenuating the patient's anxiety response to a surgical procedure can actually reduce postoperative N/V.
This study has several limitations. First, we lacked data on N/V level beyond the first 24 hours after surgery, which would have provided a better understanding of the temporal course of N/V. Second, we did not measure other potential predictors of patients' satisfaction that may have considerable influence on their overall satisfaction with the ambulatory hand surgery setting, including the patient's physical or mental state, the waiting or admission time, the medical staff's explanation and the accessibility of the medical facility. Third, we excluded patients that underwent regional anesthesia, as regional anesthesia is not generally thought to be associated with postoperative N/V. However, this could have resulted in selection bias in our patients. Fourth, this study found that the investigated factors accounted for only 21% variability of the postoperative N/V, leaving a large portion of variance in postoperative N/V unexplained. Finally, patients in this study might have reflected some recall bias in terms of their perioperative experience.
In summary, postoperative N/V was associated with a non-smoking history, a history of motion sickness and a high level of preoperative anxiety in patients undergoing ambulatory hand surgeries under general anesthesia. Although most of the patients were satisfied with this setting, moderate to high levels of N/V were associated with the patients' dissatisfaction with this setting, suggesting a need for better identifying and managing those patients at risk. The information regarding risk factors for N/V could help in preoperative patient consultation regarding the ambulatory hand surgery under general anesthesia.


 XML Download
XML Download