

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Most patients with high-grade osteosarcoma experience three symptomatic phases. Initially, intermittent pain often related to minor trauma lasts for 2 to 3 weeks. Pain may improve with conservative measures, which can be overlooked as a minor problem by both patients and physicians (asymptomatic period). Eventually, the pain becomes severe and a tender soft tissue mass develops approximately 2 months after the initial onset of pain. At this phase, most osteosarcomas could be readily recognized both clinically and plain radiographically.1)
Prompt treatment of malignant bone tumors may increase survival and decrease the amount of tissue resected for limb salvage. Nevertheless, in one study, the average delay from the onset of symptoms to the accurate diagnosis of osteosarcoma was approximately 15 weeks (average patient delay of 6 weeks, average physician delay of 9 weeks).2) The reasons for diagnostic delay might include failure to obtain radiograph at the initial visit, failure to recognize the radiologic findings suggesting malignant tumor during initial phase with sporadic pain, failure to suspect malignancy even though there is definite destructive changes, and failure to repeat the radiograph for follow-up. However, radiographic findings of incipient phase of osteosarcoma during the initial symptomatic period and their changes with disease progression remain unclear.
In the present study, we assessed the plain radiographic characteristics of 10 cases of osteosarcoma during their initial symptomatic period, which had been overlooked by a primary physician. The purpose of this study is to highlight the ill-informed findings of incipient-stage osteosarcoma with the aim of facilitating early diagnosis. Additionally, we assessed chronologic changes in radiographic findings between initial painful period and at time when malignant nature of the disease is evident.
METHODS
This retrospective analysis included 10 patients with osteosarcoma who were treated at our institute. The cases were selected on the basis of the availability of plain radiographs that were taken during the initial painful period (2- to 3-week duration). The clinical records of the 10 patients were reviewed for clinical parameters, including age, sex, location, presenting symptoms, initial diagnosis, duration from initial symptoms to definite diagnosis, and plain radiographic findings of the tumor. All initial radiographs were obtained from the referral institutions. Two of the 10 patients underwent magnetic resonance imaging (MRI) at the time of the initial onset of pain, and a definite diagnosis was made. In the remaining 8 patients, both initial and follow-up (when a clinical diagnosis of osteosarcoma was evident) radiographs were available. Analyzed radiologic findings on the initial plain radiographs included trabecular destruction, type of intramedullary matrix change (e.g., osteolysis, osteosclerosis, and mixed), cortical destruction, periosteal reaction, and the presence of soft tissue masses. In the 8 patients for whom both initial and follow-up radiographs were available, radiographic changes over time were analyzed. In 5 patients, preoperative chemotherapy, surgery, and postoperative chemotherapy were done as described previously.3) The remaining 5 patients underwent up-front surgery followed by adjuvant chemotherapy with identical protocol. Informed consent was obtained from all patients or their legal guardians as appropriate. This study was approved by our institutional research review board.
RESULTS
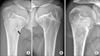
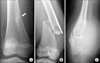
Patient characteristics and the initial radiologic findings are summarized in Table 1. The study population included 7 female and 3 male patients. Patient ages ranged from 7-26 years with an average age of 14 years. All patients presented with pain for 1-3 weeks without trauma history. In one patient (case 5), the pain developed after participating in a summer camp. Initial clinical diagnoses were sprain in 6 patients (60%), growing pains in 2 patients (20%), stress fracture in 1 patient (10%), and infection in 1 patient (10%). Two patients (cases 9 and 10) had undergone MRI when the initial pain was experienced and were diagnosed as having aggressive bone tumors. In case 9, the primary physician noticed a periosteal reaction. Under the impression of infectious condition, the physician recommended MRI and confirmed the presence of a bone tumor. In case 10, the physician recommended a conservative management; however, the patient's parents strongly requested an MRI, which revealed an unsuspected soft tissue mass (Fig. 1). In the remaining 8 patients, the time to definite diagnosis ranged from 1 to 4 months (average, 2.5 months). The initial plain radiographic findings included trabecular destruction (100%), cortical disruption (60%), periosteal reaction (60%), and soft tissue mass (10%). The observed types of intramedullary matrix changes included minimal osteosclerosis in 6 patients (60%) and faint osteolysis in 4 (40%) (Fig. 2). The plain radiographic changes after the initial symptoms and asymptomatic periods are summarized in Table 2. Surprisingly, the attending physicians still misdiagnosed osteosarcoma as other conditions in 2 of the 8 patients (cases 1 and 5). One patient (case 1) revisited the referral center with a fracture after minor trauma. The physician overlooked the possibility of a pathologic fracture and performed an internal fixation. Three months later, the patient returned with full-blown osteosarcoma (Fig. 3). The other patient (case 5), under the initial clinical impression of stress fracture, underwent cast immobilization for 3 weeks followed by physical therapy and weekly radiologic examinations. At 4 months after the initial visit, despite persistent pain and progressive swelling, the primary physician regarded the osteosarcoma as the healing stage of the stress fracture (Fig. 4). With regard to intramedullary matrix changes following disease progression, 4 cases with minimal sclerosis progressed to either osteoblastic lesions (3 cases) or osteolytic lesions (1 case). Furthermore, 4 cases with faint osteolytic foci transformed into either osteolytic lesions (3 cases) or a mixed pattern (1 case).
DISCUSSION
Most osteosarcomas at relatively advanced stages are easily diagnosed both clinically and radiologically. Typical plain radiologic features include mixed areas of lysis and sclerosis, cortical destruction, periosteal new bone formation, and soft tissue masses. However, osteosarcomas may present with diverse radiologic features that they are either misdiagnosed and underwent inappropriate procedure or rarely left undetected by primary physician.4,5,6,7,8) Misdiagnosis and inappropriate procedures are common for osteosarcomas in unusual locations that simulate benign bone tumors, fractures, and infections.9,10,11) Incipient-stage or slowly progressing osteosarcomas are sometimes not detected. We focused on the plain radiographic characteristics of osteosarcoma when patients complain initial pain for weeks. Notable radiologic findings at this stage included trabecular disruption, along with faint osteosclerosis or osteolysis. With the disease progression, these lesions progressed to typical features of malignant bone tumor.
The radiographic features of incipient- or early-stage osteosarcoma are not well known, and very few publications are available.5,9) Although the early changes of osteosarcoma are not well defined, de Santos and Edeiken5) reported that an area of trabecular destruction in the metaphysis is the most frequent finding, followed by cortical destruction, small soft tissue extraosseous masses, and occasional vague areas of increased density in the metaphysis. We also observed similar presentation patterns. Therefore, an area of trabecular destruction that accompanies changes in marrow density seems to be a principal finding of incipient-stage osteosarcoma. Additionally, if small areas of cortical destruction or faint periosteal reactions are present along with the aforementioned changes, the possibility of a malignant bone tumor should be strongly suspected.
At this early stage, whether the extent of tumor is confined to the intramedullary space or whether it has already penetrated the cortex is the issue. Although reports are scarce, patients who presented with minimal changes on the plain radiograph may reveal unsuspected extraosseous soft tissue on computed tomography or MRI.5) This may suggest that the growth pattern of osteosarcoma is double sigmoidal rather than single sigmoidal type; that is, tumors grow rapidly during the initial painful period followed by consolidation (asymptomatic period) and spurt phases (relatively advanced period).
It was interesting to note that initial minimal sclerotic lesions generally transformed to the osteoblastic type and faint lytic lesions progressed to the osteolytic type. In our previous study, because osteoblastic tumors were larger and tended to show poorer response than tumors with other patterns, we assumed that osteosarcoma might begin as a lytic lesion and gradually progress to an osteoblastic lesion.12) However, tumors with dominant sclerotic change on plain radiograph at their incipient phase tend to progress osteoblastic osteosarcoma while the opposite may be applied for osteolytic osteosarcoma. Still, this kind of observation should be confirmed in larger cases.
With regard to the issue of physician delays in diagnosis, Widhe and Widhe2) proposed three factors. Firstly, tumors in locations (spine or pelvis) that are difficult to visualize on plain radiographs. Secondly, the initial clinical impression of normal radiographic finding was accepted for too long before repeat radiographs were made. Finally, treatment for other diagnoses for too long despite the patients show different clinical picture from original (incorrect) diagnosis. In the present study, the latter two factors could account for all cases. Regarding second factor-related delay, since most osteosarcomas are diagnosed at their relatively advanced stage, it is difficult to define whether this is an actual delay or an early detection failure. In 8 patients in the present study, the primary physicians failed to detect any radiologic abnormalities, even though they compared radiographs of both affected and unaffected limbs. A possible reason for a failure to detect osteosarcoma is that the disease is too rare to elicit clinical suspicion; moreover, little information on the radiologic findings of incipient-stage osteosarcoma was given to the primary physicians and radiologists during their training courses or further education. However, delays related to the last factor could lead to catastrophic results in patients. In such cases, the primary physician often performs an inappropriate procedure under the clinical impression, such as benign bone tumor, fracture, or infection. Our previous studies indicated that an inappropriate primary procedure and a subsequent diagnostic delay have a substantial detrimental effect on the survival of osteosarcoma patients.10,13)
This study is limited by the small number of included cases. Additionally, although we conducted this retrospective analysis by meticulously collecting patient history and obtaining the relevant radiographs from the primary referral centers, variability in the lapsed time between the patient's subjective symptoms and the radiologic examination is possible.
In conclusion, the principal finding of incipient-stage osteosarcoma was trabecular disruption along with faint osteosclerosis or osteolysis. If these changes (in the absence of cortical destruction or periosteal reaction) are identified with matched clinical symptom of pain, we should perform additional tests not to miss the malignant lesion in their incipient phase.




 XML Download
XML Download