

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Rotator cuff tears are identified as among the most common causes of shoulder pain and dysfunction in adults.1,2) It is estimated that 33% of all orthopedic injuries are related to rotator cuff pathology.2-4) Clinical and cadaveric studies have shown that the prevalence of rotator cuff tears greatly increases with age. It has been reported that over 50% of patients over the age of 60 have a cuff tear and 80% of patients over the age of 80 have a cuff tear.5-8) This is compounded by occupations that require repetitive overhead activity or patients who are upper extremity dependent, as in spinal cord injury.9,10)
When conservative treatments including activity modification, physical therapy and steroid injections fail, the current standard of care for rotator cuff injury is surgical repair of the damaged tendon. Traditionally, this repair of a rotator cuff tendon tear has been performed using open or mini-open approaches. As our recent understanding of arthroscopic techniques and its instrumentation continue to improve, arthroscopic rotator cuff repair has become increasingly more popular. There have been several studies in the literature reporting successful outcomes of patients treated by arthroscopic rotator cuff repair.11-21) While maintaining rotator cuff repair integrity has been correlated to improved outcomes,22-24) the persistent tear rate after open and arthroscopic rotator cuff repair remains remarkably high.22-25) The percentage of revision surgeries has been reported to be as high as 30% for isolated supraspinatus tendon tears and 90% for large multitendon tears.23,25-27) This suggests that advances in repair techniques are needed to optimize the healing environment after repair in order to facilitate restoration of function.
Many factors contribute to an optimal repair, including repaired rotator cuff tendon-footprint motion,28) increased tendon-footprint contact area,1,29,30) and tissue quality of tendon and bone. The healing response may be reduced by intrinsic factors such as decreased vascularity, hypoxia, and fibrocartilaginous changes or extrinsic compression factors.31) Furthermore, it is well documented that torn rotator cuff muscles have a tendency to atrophy and become subject to fatty infiltration which may affect the longevity of the repair.32-36) Initial fixation strength is an essential consideration in optimizing rotator cuff repair and therefore, numerous biomechanical studies have focused on elucidating the strongest devices, knots, and repair configurations for rotator cuff repair.37-46) In addition, the initial reports demonstrated that standard arthroscopic repairs using a single-row of anchors did not adequately restore the footprint contact area.1) The technique of using two rows of suture anchors to recreate the native footprint attachment has been recently described.47,48) This "double-row" technique has been shown to closely recreate the repair site of the footprint insertion and would theoretically improve the ability of the tendon to heal to bone. A hybrid or "double-layer" technique using suture anchors medially and transosseous tunnels laterally has been shown to be stronger than repairs using suture anchors or transosseous tunnels alone in a cadaveric cyclic loading model46) and also in a sheep model loaded to failure.39) A limitation of this hybrid technique is that in clinical practice, it requires a mini-open or open approach in order to create the transosseous tunnels. Recently, Kim et al.49) reported that footprint reconstruction of the rotator cuff using two rows of suture anchors improves its initial strength and stiffness, and also decreases the gap formation and strain over the footprint when compared to a standard repair using a single-row technique. Further, recent studies have shown that a transosseous tunnel technique provides improved contact area and pressure between rotator cuff tendon and insertion footprint.1,50) Arguably, improved contact characteristics will help maximize healing potential between repaired tendon and tuberosity. In this review, the biomechanical concepts behind current rotator cuff repair techniques will be reviewed and discussed.
BIOMECHANICAL TESTING OF ROTATOR CUFF REPAIR CONSTRUCTS
Tensile testing is generally used to quantify the biomechanical characteristics/structural integrity of repaired constructs (Fig. 1). The tensile testing includes both cyclic loading and loading to failure (Fig. 2). For each cycle of the cyclic loading, two important biomechanical parameters are determined. The first parameter is the linear stiffness of the construct, defined as the slope of the linear portion of the load-elongation curve with units of N/mm. The second parameter is the hysteresis of the construct, defined as the differences in area under the loading and unloading curves on the load-elongation curve. This parameter represents energy dissipated in the construct during each cycle of loading and unloading. This energy can be dissipated in many ways, including suture anchor-bone slippage, knot slippage, and tissue fiber alignment.

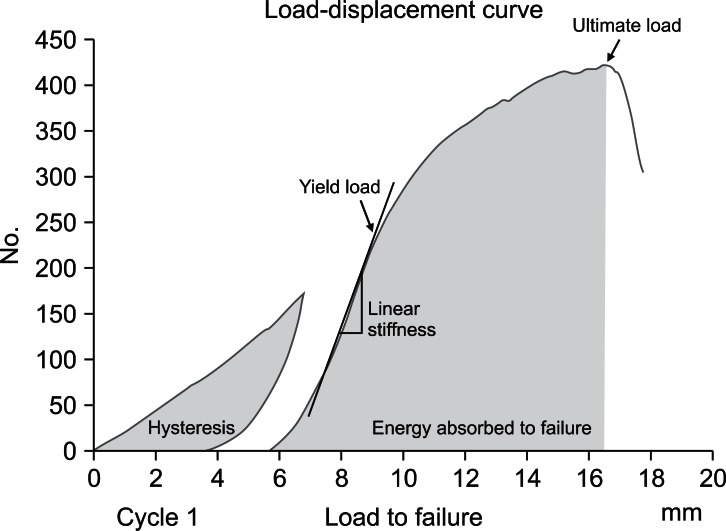
From the load to failure tests, four important biomechanical parameters are determined. The first is the linear stiffness of the construct, which is determined in the same fashion as described for cyclic loading. The next parameter is yield load and deformation, which is the load and deformation at which the load/elongation curve deviates from linearity; that is, when the stiffness begins to decrease. The yield load and deformation represents the transition point between elastic and plastic load and deformation of the construct. Prior to reaching yield load and deformation, the construct is in the elastic load and deformation range where all deformation is recoverable, but once surpassing the yield load permanent plastic deformation occurs. The next parameter is the ultimate load and deformation, which represents the maximum load and deformation sustained by the construct prior to failure. Lastly, the energy absorbed by the construct can be calculated at both yield load and ultimate load and deformation by calculating the area under the load-elongation curve. The final biomechanical parameter commonly used is gap formation which is unique to reconstructed tendon bone complex. Gap formation is the migration of the tendon edge away from the footprint with loading. It is typically measured by tracking the markers on the surface of the construct using video digitizing system.30,49,51-53)
Single-Row Repair
The treatment of rotator cuff disease progressed to arthroscopic treatment during the 1980s. The first paper to describe arthroscopic subacromial decompression and acromioplasty for chronic external shoulder impingement was Ellman's54) in 1985. However, for rotator cuff repair, the open approach with a transosseous repair was considered the gold standard. This led to the development of suture anchors and improved arthroscopic instrumentation for arthroscopic rotator cuff repairs. The first generation repair techniques involved a single-row of suture anchors placed at the lateral footprint. The suture was then passed through the torn tendon edge and the tendon was tied down to the anchor (Fig. 3). A limitation of this repair is that it relies on the lateral tendon edge for fixation, permitted footprint reconstruction only at the insertion point of the suture anchor. This inability to establish the medial-to-lateral footprint with a single-row construct was thought to be the main source for suboptimal healing rates and high re-tear rates.22) This is clearly demonstrated with the arm in abduction where the medial aspect of the tendon is lifted from the footprint. In a quantitative study, Apreleva et al.1) investigated contact characteristics for four different repair constructs. They reported that while no repair method completely restored the area of the original supraspinatus insertion, the transosseous repair restored 20% more area than any of the other repair types. This is consistent with a study by Park et al.50) in which a bovine model and pressure-sensitive film were used to assess contact characteristics of a transosseous repair versus single-row mattress configuration and single-row simple suture configuration. Once again, the mean contact area and interface pressure were significantly larger in the transosseous repair than either of the single-row constructs.
Cadaveric studies investigating transosseous repairs showed good biomechanical characteristics after repairs.28,51,53,55-57) Of these, two interesting studies were the studies by Yu et al.57) and Ahmad et al.28) The study by Yu et al.57) used cadaveric specimens already with full-thickness, U-shaped supraspinatus tears to determine the biomechanical characteristics before repair, after transosseous repair, and then after creating a complete supraspinatus tear. These authors used a three-dimensional digitizing system to detect any changes in humeral position, and they used pressure-sensitive film to assess any change in contact characteristics. With a simulated complete rotator cuff tear, they found that the humerus shifted inferiorly compared to the repaired supraspinatus tear. Interestingly, there was no increase in glenohumeral contact pressure in the repair group compared to either of the tear groups. The only measurable effect that supraspinatus repair provided was an increase in percent inferior force at 10° abduction and 60 N of load on all muscles. This increase may represent a greater concavity-compression effect, which would provide increased stability of the glenohumeral joint. Ahmad et al.28) quantified the amount of motion between the repaired tendon and bone in a transosseous repair versus a single-row construct. This is important, as the ideal repair construct would minimize motion in the immediate postoperative setting in order to allow healing of the tendon to bone. They found that the transosseous suture repair allowed less motion in internal and external rotation compared to the single-row construct.
Double-Row Repair
Double-row repair was created to increase the footprint contact area and distribute the stress over multiple fixation points. Fealy et al.47) originally described a double-row rotator cuff repair using a mini-open approach where one row of suture anchors were placed medially and another laterally. Lo and Burkhart48) then described their arthroscopic technique for a double-row repair. The first row is placed just lateral to the articular margin, then the lateral anchors are inserted just medial to the "drop-off" point of the greater tuberosity. The medial sutures are passed through the medial aspect of the tendon in a mattress fashion and tied down. The lateral sutures are then passed through the tendon in a simple suture formation and tied down. This gives medial row and lateral row fixation to increase the contact area of the repair (Fig. 4).
Multiple cadaveric studies have shown the structural integrity superiority of double-row repair compared to single-row repair. This is intuitively obvious due to the added fixation covering a larger footprint area provided by two additional anchors used in double-row fixation compared to single-row fixation. The majority of the studies49,58) showed improved biomechanical characteristics of a double-row repair compared with a single-row repair. There was significantly decreased gap formation at the first and last cycle, decreased initial strain throughout the entire footprint, as well as increased stiffness and load to failure in the double-row group. These comparisons have been evolving due to different types of rotator cuff tears and past successes of the single-row repairs. For example, with retracted chronic rotator cuff tear, Snyder59) has promoted a medialized single-row repair in order to reduce tension on the repair and promote healing. A study by Domb et al.60) compared high-tension double-row and a medialized single-row constructs. They found that the high-tension double-row repair fared better than the medialized single-row construct. There was significantly decreased displacement at first cycle, stiffness in the final cycle, and ultimate load to failure. The authors concluded that when possible, a retracted tear should be repaired with a double-row construct. A study by Ma et al.61) tested a standard double-row repair with three different single-row repairs: the Mason-Allen stitch, massive cuff stitch, and two simple sutures. The massive cuff stitch, first described by Ma et al.,43) uses a horizontal loop as a stop-stitch to prevent pullout. The double-row construct was as good as or better than all single-row repair constructs in all parameters tested.
The "double-layer" rotator cuff repair was developed by Waltrip et al.46) and was tested against a single-row construct and a traditional transosseous construct. This double-row technique used a transosseous lateral row along with a medial row of anchors. These authors used cyclic loading to test the constructs and defined failure as a 1 cm gap at the repair site. They reported that double-layer technique required significantly more cycles to fail, but there was no significant difference between the traditional transosseous construct and the single-row construct. This study was consistent with Meier and Meier,62) who compared transosseous, single-row and double-row repairs. Once again using cyclic loading and failure defined as 1 cm of gap formation, the double-row construct showed improved biomechanical characteristics compared to the other groups. The same authors also used three-dimensional mapping to analyze the footprint area restored in single-row, double-row, and transosseous constructs.63) They found that a double-row repair consistently repaired 100% of the area of the footprint, while a single-row construct only restored 46% and a transosseous repair restored only 71% of the footprint.
Finite element models were also used by Sano et al.64) to characterize stress concentration at the repair site in a single-row, double-row, and transosseous repair. In the single-row and double-row models, there was a high stress concentration on the bursal surface of the tendon and at the site of the anchors. With simulated muscle contraction, the stress moved proximally along the bursal surface of the tendon. In the double-row construct, there was more stress in the medial row of anchors than the lateral row. In the transosseous model, the highest stress concentration was seen at the cortex of the greater tuberosity and at the surface of the bony trough. With simulated muscle contraction, the highest stress stayed in the bony trough, and there was no significant concentration inside the tendon. This is advantageous for chronic rotator cuff tears with a degenerated tendon where the tendon cannot tolerate large amounts of strain.
Transosseous-Equivalent Rotator Cuff Repair
The transosseous-equivalent (TOE) or "suture-bridge" configuration was developed by Park et al.65) to provide improved contact area and pressure at the tendon footprint interface to increase healing potential. For this novel repair technique, the medial row of anchors is placed at the articular margin and the sutures are passed in a mattress fashion ideally 10 to 12 mm medial to the lateral edge of the tear. The sutures are then tied but not cut. Instead, a suture limb from each anchor is brought laterally over the "tendon bridge" and fixed using a Bio-Tenodesis screwdriver (Arthrex, Naples, FL, USA). One or two anchors can be used laterally depending on the size of the tear. The lateral fixation points are 1 cm distal to the lateral edge of the tuberosity (Fig. 5). Multiple different knotless suture anchors have been developed for lateral row fixation instead of the Bio-Tenodesis screwdriver. The major differences between the TOE and initial double-row fixation techniques are the suture bridge over the tendon and the more distal fixation points for the lateral row. The suture bridge connects the medial and lateral rows, as well as the anterior-posterior rows, allowing compression throughout the entire footprint. This highlights the difference between footprint coverage and contact pressure. While a standard double-row repair may allow the same amount of the footprint to be covered, a TOE differs from an unlinked double-row construct in that compression is throughout the entire repair instead of only at the anchor insertion points. By placing the lateral row of anchors orthogonal from rotator cuff-loading vector, a compression vector over the tendon is created to increase pressure at the footprint. This greatly increases the contact pressure along the repaired tendon in the TOE repair compared to the double-row repair.
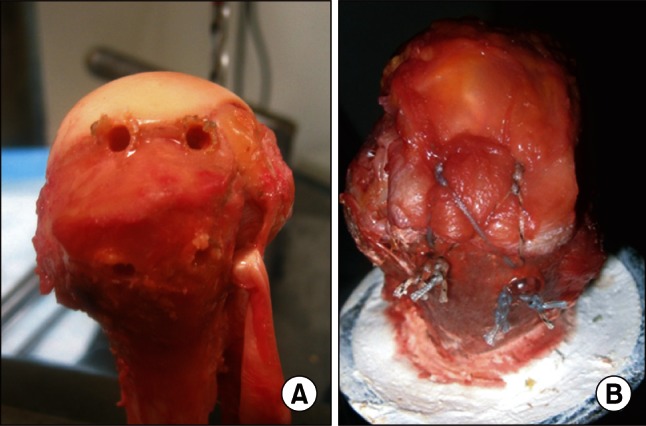 | Fig. 5Transosseous-equivalent supraspinatus repair developed by Park, et al.30) Compared to the original double-row repair, the lateral row of anchors is placed distally, allowing tensioning of the suture bridge that provides compression between the tendon and bone. (A) Anchor locations and (B) final repair.
|
In biomechanical studies by Park et al.29,30) the TOE and first generation double-row techniques were compared. These authors reported that ultimate load to failure was significantly increased in the TOE group compared to the double-row group. Gap formation and stiffness were not found to be statistically different although there was a trend towards decreased gap formation in the TOE group. They also investigated the contact characteristics of a 4-strand suture bridge versus a standard double-row repair using pressure-sensitive film. There was a significant increase in mean pressurized contact area and mean contact pressure in the TOE group.
The testing methods have also been evolving. In all prior biomechanical studies, the humerus' rotational degree of freedom was constrained. However, it has been shown that the supraspinatus can act as an internal or external rotator based on the position of the humerus.66,67) Park et al.68) also demonstrated that allowing for dynamic external rotation of the humerus with loading changes the gap formation and strain compared to the humerus fixed. They reported that external rotation produces higher gap formation and tendon strain anteriorly than posteriorly. A subsequent study by Park et al.69) tested a standard double-row construct with the TOE allowing for dynamic external rotation. They reported that the TOE had a significantly higher yield load than the double-row construct, but there was no difference in gap formation, stiffness, ultimate load to failure, and energy absorbed to failure. Within the TOE construct, they reported that significantly greater gap formation anteriorly than posteriorly, but this was not seen in the double-row group. The authors state that this is likely due to anchor placement; in the double-row construct there is an anchor placed directly at the anterolateral edge of the tear while the anterolateral anchor for the TOE is placed further distal-lateral. This study also highlights the possible need for stronger anterior fixation with the TOE In order to prevent gap formation.
The TOE techniques have also evolved and been investigated in more detail. A study by Mazzocca et al.70) used a pressure-sensitive sensor to look at different repair constructs over time. These authors tested a single-row, double-row, TOE, and suture-chain TOE. The suture-chain TOE uses FiberChain (Arthrex) to connect the medial and lateral rows, but unlike the TOE, the anterior and posterior anchors are not connected. They reported contact force, pressure and contact area immediately after repair, every minute for the first 10 minutes, every 3 minutes for the next 30 minutes, and then every 30 minutes until a total of 160 minutes. All repair techniques had decreased contact force, pressure and area at 160 minutes compared with immediately after repair, but the TOE had the highest contact pressure and force at all time points. The TOE was the only repair with a statistically significant increase in pressure and contact force when compared with the single-row construct at all time points; however, the TOE also had the greatest loss of force after 160 minutes. The contact pressure in all groups dropped at least 32% after 160 minutes. This study emphasizes the importance of a strong, stable rotator cuff repair in the immediate post-operative period, and it shows that a TOE provides the strongest initial construct and potential for healing. Within the TOE technique, Busfield et al.52) investigated the importance of the medial row knots in a TOE configuration. In both groups with supraspinatus tears, a TOE configuration was used, but in one, the medial row was fixed with a knotless suture anchor while a standard anchor with knots was used in the other group. Biomechanical testing showed greater gap formation during cyclic loading and yield load in the knotless group as well as a decreased ultimate load. Therefore, the authors concluded that a medial row of knots provides a biomechanically stronger construct compared with knotless fixation.
Go to : 
CONCLUSIONS
The rotator cuff plays an integral part in glenohumeral stability and motion. Tears of the rotator cuff alter the biomechanics, including the strain patterns of the intact cuff, which can lead to tear propagation. The goal of creating a better biomechanical construct is to increase initial fixation strength and optimize the mechanical environment for healing. While there is sure to be further evolution of repair constructs, currently the transosseous-equivalent repair developed by Park et al.65) consistently provides the best biomechanical characteristics. However, it is important to note that the ideal healing environment for these cuff repairs is still unknown.
Go to :
 XML Download
XML Download