

 PDF
PDF ePub
ePub Citation
Citation Print
Print


To the Editor:
Osteochondroma, which is the most common benign bone tumor, is an exophytic bone tumor covered by a cap of cartilage. It exists in two clinical settings, as a solitary lesion (solitary osteochondroma) and as a multiple lesion (multiple hereditary exostoses). The most common affected site is the metaphysis around the knee, especially in the distal femur. When pain or neurologic symptoms develop due to compression, resection of the tumor is recommended. The resection line is supposed to be at the base of the tumor, namely at the border with the normal bone. The recurrence of osteochondroma is rare, but it does recur in an estimated 2% of cases.1) Moreover, the development of osteosarcoma at the initial site of a treated osteochondroma has been reported.2) In addition, osteosarcoma has been reported within the stalk of an osteochondroma.3)
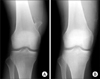
The most common resection tools are a flat chisel, a bone saw or a wire-saw. However, these tools make complete resection of an osteochondroma in the metaphysis of a lone bone difficult, due to continuity of the osteochondroma and the host bone, and because of the anatomical concave shape of the metaphysis of the host bone. In contrast, usage of a curved chisel (radius, 40 or 45 mm; length, 48.5 or 65 mm; width, 15 or 20 mm; Sonne Co. Tokyo, Japan) (Fig. 1) for transposition osteotomy of the acetabulum4) with or without an intraoperative radiograph makes complete resection of osteochondroma in the long bone easier, thereby minimizing the chance of its recurrence and reducing the possibility of the subsequent development of a malignant bone tumor (Fig. 2).

 XML Download
XML Download