

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Muscle atrophy means a gradual shrinking of the muscle tissue as a result of inactivity or disease, and atrophy of the rotator cuff muscle may occur for a variety of reasons such cuffas aging, disuse, diabetes, and suprascapular nerve injury, with the most common being chronic rotator cuff tears.1-4) It is well known that the atrophy of rotator cuff muscles is one of the most important prognostic factors for anatomic and functional results following surgical repair.5-8) Decreased postoperative strength, limited shoulder motion, and failure after tendon repair are the main clinical implications of the atrophy of the rotator cuff muscles.5,7,9,10) Atrophy of rotator cuff muscle was first quantitatively measured by Thomazeau et al.11) as the occupation ratio, which is the ratio between the cross sectional area of the muscle belly and that of its fossa on oblique sagittal Y-view of magnetic resonance imaging (MRI). The correlation of the occupation ratio between MRI and multidetector computed tomography (MDCT) was validated in our previous study.12)
To date, even though some studies suggest that surgical cuff repair may halt the atrophy of rotator cuff muscles,9,11) it has been considered an irreversible phenomenon, and the function of the shoulder joint remains impaired, especially in higher stages of atrophy.5,6,13,14) However, we do observe recovery of the atrophy of rotator cuff muscles on a regular follow-up examination after surgical repair, and the question is whether the atrophy is truly irreversible after rotator cuff repair.
The hypothesis of this study is that the atrophy of rotator cuff muscles can be improved after surgical repair. We investigated whether there was a significant improvement of the supraspinatus muscle atrophy postoperatively by comparing the pre- and postoperative occupation ratios. We further assessed the factors associated with the possible improvement of the atrophy.
METHODS
Demographics
This was a retrospective study. Among 412 patients who underwent surgical cuff repair for full-thickness rotator cuff tears confirmed by arthroscopic findings at the authors' institution between January 2005 and July 2008, 191 patients who underwent both preoperative MRI and postoperative MDCT at least one year after the operation were included. The postoperative MDCT was performed at a mean of 13.2 ± 3.8 months after operation (range, 12 to 16 months), without special indication. We excluded patients with isolated subscapularis tear (n = 5), previous operation on the same shoulder joint (n = 4), and incomplete repair (n = 6). Patients who did not have preoperative MRI (n = 8) or postoperative MDCT (n = 166), and those with MRI or MDCT images that were not usable due to poor quality or absence of appropriate Y-view were also excluded (n = 32). Most of the patients without the postoperative MDCT underwent ultrasonography as a postoperative imaging modality instead of MDCT (136 of 166), and thirty patients refused to undergo either ultrasonography or MDCT. There were no special criteria for the selection of postoperative imaging modality; however, ultrasonography was usually performed for those with financial difficulties. The average age at the time of operation was 59.7 ± 7.9 years (range, 39 to 80 years), and the postoperative MDCT was performed at a mean of 13.2 ± 3.8 months after operation. The demographic and clinical data were summarized in Table 1. We obtained the institutional review board approval for the study protocol.
Surgical Procedures
All surgical procedures were conducted by one senior author (JHO). Subacromial decompression and acromioplasty were performed to create a flat acromion. Distal clavicle resection was performed on the patients who experienced symptomatic acromioclavicular arthritis. Biceps tenotomy or tenodesis was performed for a symptomatic biceps tear involving greater than 50% of the tendon and for a symptomatic degenerative superior labral anterior and posterior (SLAP) lesion according to age or activity level of the patient. The operative technique was arthroscopic repair, mini-open repair, or open repair according to the arthroscopy learning curve and arthroscopical reparability. Repair technique was either single or double row according to the tear size, tendon status, and tear configuration and reparability. All knots were tied securely using a self-locking, sliding knot.
Immobilization after cuff repair was maintained with an abduction brace, and duration of immobilization was based on tear size as measured at the time of operation, from 4 weeks to 6 weeks. Passive motion was performed immediately after the operation, except in cases of large-to-massive tears. Active-assisted range of motion exercise was allowed after the weaning of the brace. Muscle strengthening exercises began between 9 and 12 weeks, and sports activities were permitted at 6 months after the operation.
MRI and MDCT
Even though MRI still remains the standard preoperative imaging modality for evaluation of rotator cuff, MDCT has been widely used recently for its advantages, such as cost-effectiveness, short examination time, and absence of foreign body artifact in the postoperative evaluation for patients who have undergone rotator cuff repair surgery. Our previous study showed that MDCT arthrography (MDCTA) is a very valuable method to confirm postoperative integrity after rotator cuff repair using suture anchors.15)
As such, we have used MRI as a preoperative imaging modality and MDCT as a postoperative imaging modality. MRI was performed on the Gyroscan Intera 1.5-T system (Philips Medical Systems, Utrecht, the Netherlands). From the MRI examination, we obtained T1-weighted and T2-weighted spin-echo oblique sagittal images parallel to the joint surface of the glenoid. CT was also performed using a 16-multidetector CT system (Mx8000 IDT, Philips Medical Systems). We generated oblique sagittal reconstruction images as well as oblique coronal and axial images at a three-dimensional workstation. The oblique sagittal images were reconstructed parallel to the glenohumeral joint surface, same as the MRI oblique sagittal images. The patient positioning for MRI and MDCT examinations was also same with the arm placed alongside the body in a neutral supine position.
Measurement of the Atrophy Using Photoshop on MRI and MDCT
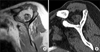
The supraspinatus muscle atrophy was measured on the same scapular Y-view of the oblique sagittal images of MRI or MDCT at the location where the body of the scapula, scapular spine, and medial border of the coracoids process form a Y-shape (Fig. 1). We defined the atrophy by calculating occupation ratio according to the method of Thomazeau et al.,11) the ratio between the cross-sectional area of the supraspinatus muscle and the supraspinatus fossa on the scapular Y-view. The boundary of the supraspinatus fossa was defined as the area from the inner margins of the Y-shape to the inner limit of the clavicle and the acromion. Originally, the occupation ratio is measured on the picture archiving and communications systems (PACS) workstation by drawing the boundary of the supraspinatus muscle and supraspinatus fossa.11) However, this method is limited in its accuracy and reliability for measuring occupation ratio, because the outlining process is conducted by subjective manual hand drawing. For that reason, in our previous study,12) we introduced a new measuring method for the supraspinatus muscle atrophy using the Photoshop software (magic selection tool, Adobe Systems Inc., San Jose, CA, USA), which is the method that automatically designates the regions of interest and calculates the number of pixels in the selected area. With the Photoshop method, we solved the reliability issue for the measurement of the atrophy, showing very high intra- and interobserver reliability: interclass correlation coefficient (ICC) of 0.89 to 0.96, 0.90 to 0.98, and 0.85 to 0.97 for intraobserver correlation on MDCT and both MR T1- and MR T2-weighted images (MRT1W and MRT2W); and ICC of 0.89, 0.92, and 0.91 for interobserver correlation, respectively (all p < 0.001). Further, we demonstrated a significant correlation between MRI and MDCT with Pearson's correlation coefficient (PCC) of 0.78 to 0.87 between MDCT and MRT1W and 0.73 to 0.82 between MDCT and MRT2W (all p < 0.001). We showed it was possible to compare the occupation ratio between MRI and MDCT by using very good-fitting regression equation derived from linear regression analysis, Y = 0.03 + 0.98X (X is the occupation ratio of MRI; and Y is that of MDCT, R2 = 0.76). Using this Photoshop method, we measured the cross-sectional area of the supraspinatus muscle and supraspinatus fossa on the Y-view, and by dividing the cross-sectional area of the supraspinatus muscle by that of the supraspinatus fossa, we calculated the occupation ratio (Fig. 2). A ratio above 0.6 was considered to be normal or mild atrophy; between 0.4 and 0.6, moderate atrophy; and below 0.4, severe atrophy.16)
Evaluation of the Change of the Atrophy Using Regression Equation
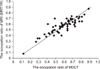
Correlation between MRI and MDCT was excellent and reliable in both MRT1W and MRT2W; however, since the correlation of MRT1W was slightly better than MRT2W,12) we used the measurements of MRT1W in this study. For the comparison of pre- and postoperative atrophic change, we first calculated the modified occupation ratio after inputting the preoperative occupation ratio measured on MRT1W into the regression equation, Y = 0.03 + 0.98X (R2 = 0.76) (Fig. 3).12) For example, an occupation ratio of 0.48 based on MRT1W is converted into 0.50 (modified occupation ratio) based on MDCT. Then, we compared this modified occupation ratio with the occupation ratio measured on postoperative MDCT. Although the measurement of occupation ratio using the Photoshop method is very accurate and reliable, because it designates the regions of interest automatically with excellent MRT1W-MDCT correlation,12) there may be some errors with the measurement. Thus, we set a possible error range of plus or minus 10%; that is, we defined the improvement of atrophy as more than a 10% increase in occupation ratio and the worsening of atrophy as more than a 10% decrease. We decided that plus or minus 10% was enough to take the measurement error into account, as the mean value of intraobserver relative error was ± 3.03%. Therefore, if the modified occupation ratio was 0.50, only an occupation ratio measured on postoperative MDCT of higher than 0.55 or lower than 0.45 was regarded as meaningful and then further classified into either the improved atrophy group or worsened atrophy group, respectively.
Evaluation of the Factors Related with the Change of the Atrophy
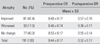
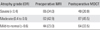
We evaluated the postoperative change of the atrophy, and performed stratification analysis according to age, retraction length, and initial degree of atrophy. The age was stratified into < 55 years, 55 to 65 years, and > 65 years; retraction length into small (< 1 cm), medium (1 to 3 cm), and large-to-massive (> 3 cm) size; and initial degree of atrophy into the occupation ratio below 0.4 (severe atrophy), between 0.4 and 0.6 (moderate atrophy), and above 0.6 (mild atrophy or normal).
In addition, we assessed various factors such as age, gender, side of involvement, tear size of both anteroposterior (AP) dimension and retraction, quality of rotator cuff muscles, symptom duration, smoking, diabetes, steroid injection, level of sports activity and demand of shoulder activity which may affect to the change of the atrophy, and the association between the change of the atrophy and cuff integrity after surgical cuff repair. The tear size in the AP dimension was measured at the lateral edge of the footprint, and retraction length was estimated by the distance from the apex of the tear to the footprint. The quality of rotator cuff muscles was evaluated by global fatty degeneration index, which is the mean grade of fatty degeneration of the supraspinatus, infraspinatus, and subscapularis described by Goutallier et al.6) The level of sports activity and the demand of shoulder activity were recorded as high, medium, and low. High level of sports activity was defined as enjoying dynamic or contact sports (e.g., boxing, rugby, basketball, football, volleyball, tennis); medium level, enjoying static sports (e.g., golf, yoga, swimming, bicycle, running); and low level, rarely playing sports. High demand of shoulder activity during work was defined as heavy manual labor; medium demand, manual labor with less activity; and low demand, sedentary worker.
In the MDCT interpretation for the integrity of the repaired supraspinatus tendon, a successful healing was defined as maintenance of the insertion into the footprint, whereas failed healing was taken as a discontinuity at the footprint. The contrast media leakage with maintenance of the cuff insertion into the footprint was not considered a failure of healing, as other authors presented.17) Experienced musculoskeletal radiologists, who were unaware of the present study, performed and interpreted the MDCT, and further evaluated the rotator cuff healing to the greater tuberosity.
Statistics
Descriptive statistics were used to report the frequency of the improvement or worsening of the supraspinatus muscle atrophy after surgical cuff repair. The paired t-test was used to compare the change of the atrophy between pre- and postoperative occupation ratios. The pre- and postoperative occupation ratios followed normal distribution (p = 0.191 and 0.100, respectively, in Kolmogorov-Smirnov test). To determine the differences between the improved atrophy group and the worsened atrophy group, Student's t-test was used for the continuous variables, and χ2 or Fisher's exact test was used for the categorical variables. For all statistical analyses, SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) was used, and p < 0.05 was considered statistically significant.
RESULTS
The atrophy measured as occupation ratio significantly improved from 0.44 ± 0.17 (range, 0.11 to 0.89) preoperatively to 0.52 ± 0.17 (range, 0.13 to 0.91) postoperatively (p < 0.001) (Fig. 4). The number of patients whose postoperative occupation ratio increased by more than a 10% (improved atrophy group) was 81 (42.4%), and the number of patients with decreased occupation ratio of more than a 10% (worsened atrophy group) was 33 (17.3%) (Table 2). The overall composition of the patients with respect to the occupation ratio was changed from low occupation ratio (severe atrophy) to high occupation ratio (mild atrophy-to-normal, p < 0.001) (Table 3).
Even after stratification, the atrophy improved regardless of age, retraction length, or initial degree of the atrophy in all cases, although small retraction (< 1 cm) and mild-to-normal initial atrophy (occupation ratio > 0.6) did not reach significant levels. However, with respect to the repair integrity, the occupation ratio was slightly decreased (atrophy was worsened) in patients whose cuffs were failed to heal after surgical repair, even though the change was not significant (Table 4).
There was no significant difference in every demographic and clinical factor between improved and worsened atrophy group; however, the proportion of unhealed cuffs was significantly higher in the worsened atrophy group (48.5%, 16 of 33) compared with the improved atrophy group (22.2%, 18 of 81, p = 0.007) (Table 5).
DISCUSSION
One of the main causes of the atrophy of the cuff muscles is rotator cuff tear.10,18) The degree of the atrophy depends on several factors such as the size of the tear, aging, and disuse, and it can lead to the loss of shoulder function including decrease in strength and failure of cuff healing after surgical repair.8,19,20) Many authors have shown that muscular atrophy is the most important prognostic factor for arthroscopic repairs of rotator cuff tendons.5,6,10,14)
Unfortunately, the atrophy progresses throughout the nonoperative treatment of rotator cuff tears,7) and even after structurally successful surgical tendon repair, it has been suggested that the rotator cuff does not recover from the atrophy.5,13,14) These studies asserted that in grade 2 or higher fatty degeneration, using the Goutallier classification,2) the muscle condition undergoes irreversible change, resulting in permanent loss of muscle function including decrease in muscle strength and an increased rate of secondary tear.
However, two studies have suggested the possibility of the improvement of the muscular atrophy. Gerber et al.9) showed that the muscular atrophy in cases of massive rotator cuff tear was at least stopped and might be reversed in successfully repaired supraspinatus musculotendinous units at least within two years. They showed that, for patients with successful repair, the increase in cross-sectional area of the supraspinatus almost reached significance (p = 0.054). In addition, Thomazeau et al.11) reported a reversal of supraspinatus atrophy in half of the successfully repaired cuffs. These two studies support the possibility of the improvement of the atrophy after effective tendon repair. However, the significance of both is limited due to a small number of included cases: 29 cases for the study of Gerber et al.9); and 30 cases for Thomazeau et al.11)
For that reason, we investigated the change of the supraspinatus muscle atrophy with a large number of cases (191 cases) using a very accurate and reliable measuring method12) in the present study, and detected a high percentage of the improvement of the atrophy (42.4%), assessed at a mean of 13.2 ± 3.8 months after operation. The atrophy improved regardless of age, retraction length, or initial degree of atrophy, although a small retraction and initial mild-to-normal atrophy (occupation ratio > 0.6) did not reach a significant level. We are quite convinced of the results, as we used a highly accurate method for the measurement of the supraspinatus muscle atrophy. The method was nearly automated and showed high interobserver (ICC, 0.89 and 0.92 on MDCT and MRT1W, respectively) and intraobserver (ICC, 0.89 to 0.96 and 0.90 to 0.98 on MDCT and MRT1W, respectively) reliabilities, with an excellent MDCT-MRT1W correlation (PCC, 0.78 to 0.87 between MDCT and MRT1W, R2 = 0.76, p < 0.001).12) We also applied very strict criteria for the definitions of the improvement and worsening of the atrophy (more than a 10% difference in occupation ratio).
We consider that the mechanical reloading may play a role for the improvement of the muscular atrophy after surgical cuff repair. Torn cuffs, without effects of mechanical stress from the proximal humerus, will consequently lead to fatty infiltration or atrophy of cuff muscles.18,21) The prolonged load-deprivation status of torn cuff muscles may be similar to that of disuse or immobilization, and skeletal muscle atrophy in such conditions has been well demonstrated in many studies.22,23) On the contrary, cuff muscles may be mechanically reloaded after surgical cuff repair, possibly stimulating protein synthesis in atrophied cuff muscles and eventually resulting in recovery of muscular mass and decrease of fatty infiltration.24) Many factors have been suggested to be related to the initiation of protein synthesis from mechanical loading of the muscle. Recent data have shown that mechanical loading of the muscle membrane may induce activation of the mammalian target of rapamycin (mTOR), which stimulates the initiation of protein synthesis.25) In addition, a number of cytokines including leukemia inhibitory factor, insulin-like growth factor, and integrin have been suggested to have the ability to contribute to loading-induced muscle hypertrophy.26-28) Also, we think that the change in the pennation angle after surgical cuff repair may be another mechanism for the improvement of the muscular atrophy. Some authors have suggested that retraction of the muscle belly as a result of full-thickness rotator cuff tear could lead to a change in the pennation angle between the muscle fibers, and this altered angle might allow fat to infiltrate between the fibers of muscle and produce atrophy of the rotator cuff muscle.29) Therefore, it is possible that the recovery of pennation angle via surgical cuff repair may induce a decrease in the amount of fatty tissue between the muscle fibers and an improvement of muscular atrophy. Gerber et al.29) demonstrated that continuous elongation and repair of a retracted and atrophied rotator cuff muscle can lead to a restoration of the normal pennation angle, partial reversal of muscle atrophy, and arrest of the progression of fatty infiltration in the animal study using sheep.
The failure rate of cuff healing was significantly higher in patients whose atrophy was worsened postoperatively (48.5%), compared with those with improved atrophy (22.2%) in this study. Initial atrophy of the cuff muscles is a well-known prognostic factor for the anatomical results following cuff repair.6,9,30) However, it is interesting that not only initial atrophy but also postoperative change of the atrophy is a prognostic factor for structural healing after cuff repair. Moreover, while the postoperative atrophy improved distinctly in every other condition except the failure of cuff healing, patients with unhealed cuffs showed worsened atrophy postoperatively, though it was not statistically significant. Thus, we can say that not only do the unhealed cuffs show more severe atrophy than healed cuffs (the mean occupation ratios were 0.39 ± 0.14 and 0.59 ± 0.14 in this study, respectively; p < 0.001), as many other authors have demonstrated,6,9,14) but also the cuffs themselves become more atrophied or at least not improved postoperatively if the cuffs fail to heal after surgical repair. Such is consistent with the results of previous studies that stressed the importance of successful cuff repair with the more severe atrophy and poorer function in patients with unhealed cuffs.6,9,13)
There are several limitations of the current study. First, we evaluated the change of the supraspinatus muscle atrophy alone. In our previous study, we revealed that the infraspinatus muscle atrophy was the most independent prognostic factor for anatomic outcome.10) There have also been other studies which stress the influence of the infraspinatus muscle atrophy on the functional and anatomic outcomes after rotator cuff repair.6) Therefore, it is necessary to evaluate other cuff muscles such as the infraspinatus muscle, in addition to the supraspinatus muscle. However, the occupation ratio we have measured is defined only for the supraspinatus muscle, and it is almost impossible to measure the occupation ratio accurately in the other cuff muscles, as they are not surrounded by bony structure and the outer margin of the muscles is not distinct. We wanted to focus on the change of the supraspinatus muscle atrophy, which we can evaluate accurately by using our method. In addition, the fact that tear retraction can influence occupation ratio measured at one cross-sectional image is a known limitation regarding the measuring method currently used.14) While our measuring method using Photoshop overcame the weakness of previous methods with regard to accuracy and reliability,12) it also measured the occupation ratio with one cross-sectional image of the Y-view, as in other current methods which measure the atrophy of cuff muscles.11,16) Such may not well represent the condition of the entire muscle. This one cross-sectional area of the supraspinatus muscle may be influenced by retraction of the torn supraspinatus muscle.11) However, there is no widely accepted volumetric measuring method for the atrophy of rotator cuff muscles, and all studies asserting the atrophy of the rotator cuff muscles to be irreversible and worsening after successful repair have measured and compared it at a scapular Y-view, same as our study.5,14) As such, our results revealing a significant improvement of the supraspinatus muscle atrophy in a large proportion after successful cuff repair, assessed at the same scapular Y-view, may be valuable. Another limitation of the study may be the difference in the occupation ratio measured in two different imaging tools. We have compared the modified values derived from the linear regression equation and applied strict criteria of above or below 10% change of the occupation ratio. Finally, not all patients who underwent surgical repair of full-thickness rotator cuff tear were included, as we limited the patients to those who underwent both preoperative MRI and postoperative MDCT with an appropriate Y-view. Some patients refused MDCT postoperatively, because they did not want the rather expensive and time-consuming procedure. This drop-out from the cohort may cause the risk of selection bias of which we are not aware. A well-organized, randomized prospective trial may be needed to confirm our results.





 XML Download
XML Download