

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Varus deformity is the most common angular contraction for primary total knee arthroplasty (TKA).1) Anatomically, varus arthritic knees are characterized by cartilage and/or bone loss in the medial compartment. Furthermore, ligaments and soft tissues on the medial side undergo contracture, and thus, must be released to achieve neutral limb alignment in TKA.2,3) In practice, it is difficult to achieve neutral alignment when performing TKA in severely varus-deformed knees, and many studies have suggested for the addressing of severe varus deformity, subperiosteal release of the superficial medial collateral ligament (MCL),4,5) joint line release of the MCL,4) and epicondylar osteotomy.4,6) However, after performing medial soft tissue release to achieve neutral limb alignment in severely varus-deformed knees, it is difficult to balance the gap due to an abrupt increase in medial flexion gap, which can have many adverse effects after TKA, such as thicker polyethylene insert or a more constrained prosthesis use.7) In our previous study using a navigation system, we suggested that the degree of preoperative varus deformity, measured using the preoperative mechanical axis angle (MAA), and reducibility of varus deformity, measured using the valgus stress angle (VSA), influence the amount of medial soft tissue release required to achieve neutral alignment. In particular, preoperatively determined reducibility of varus deformity (based on preoperative VSA) was found to be more predictive of a medial flexion gap increase after medial release than preoperative MAA.8) Verdonk et al.1) also suggested that the reducibility of a deformity can be estimated preoperatively using stress radiographs. However, in some cases, we were unable to predict the amount of medial soft tissue release required by the measuring of preoperative VSA only.
We hypothesized that a number of clinical and radiologic parameters, such as age, body mass index (BMI), sex, duration of pain, preoperative range of motion (ROM), preoperative MAA, preoperative mechanical tibial angle (MTA), preoperative mechanical femoral angle (MFA), size of medial osteophytes, and the amount of medial femorotibial joint space narrowing, might be correlated with preoperative VSA and could influence the reducibility of varus deformity. The aims of this study were to identify the factors correlated with the reducibility of varus deformity and to predict more accurately the extent of medial soft tissue release using preoperative VSA.
METHODS
We retrospectively reviewed 181 knees in 131 patients that had undergone navigation-guided primary TKA from September 2006 to December 2009 at our institute. Of these 181 knees, 143 knees (102 patients) were as follows: with preoperative varus mechanical axis alignment; femorotibial osteoarthritis (OA) checked using preoperative radiographs; and acceptable intraoperative mechanical axis alignment (within ± 3° of neutral alignment), as determined using a navigation system and acceptable radiograph, in which patella was shown in the middle of knee joint. These 143 knees constituted the study cohort. All arthroplasties were performed by a single surgeon using a navigation system (OrthoPilot, B. Braun Aesculap, Tuttlingen, Germany), which is an image-free system that uses kinematic analysis of the hip, ankle, and knee joints, and anatomic registration of the knee joint to construct a working model of the knee. The e.motion ultra-congruence (B. Braun Aesculap, Tuttlingen, Germany) implants were used throughout.
Radiographic Evaluations
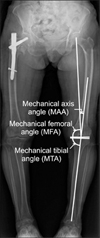
Preoperative varus deformity was assessed radiographically using a standing anteroposterior (AP) radiograph of the whole lower extremity and an AP valgus stress radiograph of the knee, taken while a valgus stress of 15 lb (6.8 kg) was applied to the knee in extension using a Telos SE arthrometer (Fa Telos, Medizinisch-Technische, Greisheim, Germany). In the text book of Noyes and Barber-Westin,9) they described that testing load (15 lb, 67 N) was required for valgus stress radiograph. Midpoints of the distal femoral shaft, which are 10 and 15 cm from the knee joint line, respectively, and the midpoints of the proximal tibial shaft, which are 7.5 and 12.5 cm from the knee joint line, were also assigned and connected on each AP valgus stress radiograph.3) The angle between these two lines was defined as the VSA (Fig. 1). In each case, knee mechanical axis was assessed preoperatively using the hip-knee-ankle angle, determined using a standing AP radiograph of the whole lower extremity.1) The hip center, femoral notch center, and ankle center were also assigned and connected, and the angle between these lines was defined as the MAA of the knee. In addition, the MTA and MFA were recorded. The MTA was defined as the medial angle between the mechanical axis of the tibia and a line tangential to the tibial plateau. The MFA was defined as the medial angle between the mechanical axis of the femur and a line tangential to the distal femoral condyle (Fig. 2).1) Standing AP radiographs of the knee were taken with both knees in extension. Femoral osteophyte size, tibial osteophyte size, and combined osteophyte size (the sum of femoral and tibial osteophyte sizes) were measured. Osteophyte size was defined as the largest perpendicular distance from the cortical line to the outer margin of an osteophyte (Fig. 3).10) Radiographic severity of medial femorotibial OA was determined using the Ahlbäck grading scale,11) which places an emphasis on joint space width. According to this scale, grade I indicates joint space narrowing (< 3 mm), grade II joint space obliteration and near obliteration, grade III minor bone attrition (0 to 5 mm), grade IV moderate bone attrition (5 to 15 mm), and grade V severe bone attrition (> 15 mm). All measurements were made by two investigators (JGK, JHH), unaware of flexion and extension gap results, by consensus using a PACS system (Centricity, GE, Chicago, IL, USA).
Surgical Procedure
The anterior and posterior cruciate ligaments were sacrificed, and the medial meniscus and osteophytes were removed after a standard medial parapatellar arthrotomy with median skin incision. Minimal medial release was carried out before registration and bone cutting in accord with preoperative VSA. When preoperative VSA was in an acceptable range (7° or more, if correctable), medial release was not performed at this stage. The femoral and tibial trackers were mounted on proximal tibia and distal femur. After marking all reference points, the navigation system was used to check for acceptable limb alignment, which ranged from a mechanical axis alignment of 3° of valgus to 3° of varus. At this stage, modified medial soft tissue release was performed, if required. Initially, the PCL was removed from its femoral and tibial attachment sites, and the medial soft tissue and posteromedial capsule were then released from the edge of the tibial joint surface. This included release of the attachment of the deep MCL. In addition, medial osteophytes were removed. If acceptable alignment was not obtained, further subperiosteal release of the superficial MCL was performed using a periosteal elevator. Otherwise, partial release of the tibial insertion of the semi-membranous was performed until an acceptable range of coronal alignment was achieved; but the pes anserinus was not released at the tibia. A tensor with a slide ruler, which allowed medial and lateral compartments to be separately adjusted, was then inserted into the space between femur and osteotomized tibia, and distraction force was applied using a laminar spreader by the surgeon using maximum right hand grip (40 kg) in extension and at 90° of flexion. Medial and lateral gaps during extension and at 90° of flexion were then recorded.8)
Evaluation of Data
Gaps in extension and in 90° of flexion and femoral component rotations recorded by the navigation system, clinical parameters, and radiographic parameters were all recorded. Correlations between the above-mentioned 12 parameters (except gender) and preoperative VSA were analyzed statistically, using Spearman's rank correlation rho. In addition, correlations among the radiologic parameters were analyzed using Spearman's rank correlation rho and Pearson's product moment correlation coefficients. To clarify the effect of parameters found to be correlated with preoperative VSA on the amount of medial release required to make acceptable intraoperative mechanical axis alignment, we allocated patients, with a preoperative VSA of ≤ 3° of valgus, into two groups. In the previous study,8) the cutoff value with extensive medial soft tissue release of ≤ 3.15° resulted in sensitivity of 96% and specificity of 73%. The two groups were: group A (28 knees), in which the difference between the lateral and medial flexion gaps (LFG - MFG) was ≤ 1 mm; and group B (23 knees), with a LFG - MFG of > 1 mm. Comparisons of parameters in groups A and B were performed using the two sample t-test, the Mann-Whitney test, Fisher's exact test, and chi-square test. A p-value of < 0.05 was considered statistically significant. All data were analyzed using SAS ver. 9.1.3 (SAS Inc., Cary, NC, USA).
RESULTS
The preoperative clinical and radiological parameters, and their correlations with the preoperative VSA are shown in Table 1.
Correlations between Preoperative Clinical Parameters and Preoperative VSA
Mean patient age was 66.6 ± 6.2 years (range, 50 to 80 years). There were 15 men and 128 women, and all had osteoarthritis of the knee. Mean preoperative knee flexion contracture was 8.1° ± 5.8° (range, 0° to 25°), and the mean preoperative knee maximum flexion angle was 132.2° ± 13.5° (range, 95° to 150°). Mean duration of pain was 9.7 ± 7.1 years (range, 0.5 to 30 years). Mean BMI was 27.1 ± 3.2 kg/m2 (range, 17.5 to 37.0 kg/m2). No association was found between these parameters and preoperative VSA.
Correlations between Preoperative Radiologic Parameters and Preoperative VSA
Mean preoperative MAA was 10.3° ± 4.6° varus (range, 5° to 28.1° varus), and mean preoperative VSA was 4.6° ± 3.0° valgus (range, 0.0° to 14.7° valgus). Mean MTA was 85.3° ± 3.6° (range, 75° to 94.1°), and mean MFA was 87.7° ± 4.2° (range, 68° to 98.0°). Mean femoral osteophyte size was 4.4 ± 1.7 mm (range, 0 to 9.4 mm), mean tibial osteophyte size was 3.5 ± 1.6 mm (range, 0 to 9.3 mm), and combined osteophyte size was 8.0 ± 3.0 mm (range, 0 to 17.2 mm). According to the Ahlbäck grading scale, 57 knees (39.8%) were graded as I, 29 knees (20.2%) were graded as II, 56 knees (39.1%) were graded as III, and one knee (0.6%) was graded as IV, preoperatively. No case was graded as V preoperatively. A negative correlation was found between preoperative MAA and preoperative VSA (p < 0.01, r = -0.38), and a positive correlation was found between preoperative MTA and preoperative VSA (p = 0.01, r = 0.19). However, no association was found between the other parameters and preoperative VSA (Table 1).
Correlations among Preoperative Radiologic Parameters
Negative correlations were found between preoperative MTA and MAA (p < 0.001, r = -0.33), and between preoperative MTA and MFA (p < 0.001, r = -0.51). However, no significant correlation was found between preoperative MTA and the other radiologic parameters (osteophyte size and the Ahlbäck grading scale). A negative correlation was found between preoperative MAA and MFA (p < 0.001, r = -0.20), and positive correlations were found between the Ahlbäck grading scale and femoral osteophyte size (p < 0.001, r = 0.25), tibial osteophyte size (p = 0.02, r = 0.17), and combined osteophyte size (p < 0.001, r = 0.25).
Comparison of Group A and B with Respect to Radiologic Parameters
Mean preoperative MAA values in group A and B were 13.6° ± 5.4° varus (range, 3.7° to 28.1°) and 11.2° ± 3.0° varus (range, 5.8° to 17.4°), respectively. Mean preoperative MAA values were found to be significantly different in the two groups (p = 0.03); and mean preoperative MTA values were 83.2° ± 3.7° (range, 75.0° to 90.6°) and 85.3° ± 3.3° (range, 78.2° to 92.5°) in groups A and B, respectively. These values were significantly different by the two sample t-test (p = 0.03). Preoperative osteophyte size, preoperative MFA, and the Ahlbäck grading scale were not significantly different in the two groups groups (Table 2).
DISCUSSION
Our principal findings of the present study were that degree of varus deformity and proximal tibial vara (measured by preoperative MAA and MTA, respectively) were factors correlated with reducibility of varus deformity (measured by preoperative VSA), and that clinical parameters and other radiologic parameters (osteophyte size, severity of OA, and angulation of distal femoral joint surface) were not significantly correlated with reducibility of varus deformity. In our previous study, we suggested that the reducibility of varus deformity was more important an factor affecting the degree of medial release and recommended preoperative VSA, as an indicator of determining the degree of medial release.8) However, some knees with a small preoperative VSA (suspected of poor varus deformity reducibility) were corrected without excessive medial release in TKA. As such, we wondered what factors were correlated with preoperative VSA. As far as we knew, there was no study analyzing the factors affecting the reducibility of varus deformity.
Saragaglia et al.12) emphasized that navigation reduced the incidence of extensive soft tissue release. However, we were able to prevent excessive medial soft tissue release during varus deformity TKA by using preoperative VSA and navigation together. Orthopedic surgeons have assessed ligament balance in three stages during surgery: stage I under general anesthesia; stage II after distal femoral cutting; and stage III after proximal tibial cutting.12) Preoperative VSA could be used in stage I. As mentioned above in our description of the surgical procedure, minimal medial release is carried out before navigation registration and bone cutting to correct varus deformity in accord with preoperative VSA. At stages II and III, navigation guided TKA provides surgeons the permanent access to gap balance and the mechanical axis for reference purposes with impression of varus deformity acquired by preoperative VSA.13) As excessive medial release can be avoided based on impressions obtained during surgery, preoperative VSA provides information as valuable as the navigation system.
Several studies have concluded that medial flexion gap increases more after extensive medial soft tissue release, especially the superficial MCL, during varus deformity TKA.3,14-16) When the medial gap increases or becomes larger than the lateral gap in flexion, the difference between LFG-MFG decreases or sometimes becomes negative. Therefore, by using gaps in 90° of flexion recorded by the navigation system, we allocated patients to two groups according to the extent of medial soft tissue release. Group A was with LFG-MFG ≤ 1 mm; and in group B, LFG-MFG was > 1 mm. In our previous study, we suggested that preoperative varus deformity measured using preoperative MAA and VSA values was associated with a medial flexion gap increase, when extensive medial soft tissue release was performed to achieve neutral alignment. Furthermore, preoperatively determined reducibility of varus deformity (based on preoperative VSA) was found to be more predictive of a medial flexion gap increase after extensive medial release than preoperative alignment based on preoperative MAA.8)
In experimental models of OA, osteophyte formation in unstable joints was found to be promoted by joint movement, and it was suggested that osteophytes must grow laterally to widen joint surfaces, and thus, stabilize joints.17) Some authors have suggested that osteophytes developed in articular surface regions where stress has been reduced due to alterations in joint architecture.18,19) Pottenger et al.20) found that osteophyte removal during TKA for knee OA increased instability. It suggests that osteophytes are able to stabilize the OA joint, and that osteophytes in the OA involved compartment may increase stability by pressing directly against slackened collateral ligaments. Thus, ligament contracture and osteophyte appear to stabilize osteoarthritic joints. We considered that osteophyte are likely to be related to preoperative VSA, and that varus deformity could be corrected without excessive medial soft tissue release, after removing large osteophytes. However, our results show that osteophyte size is not correlated with preoperative VSA or the amount of medial soft tissue release. Pottenger et al.20) showed that varus-valgus angle increased by 3.6° for each centimeter of ipsilateral femoral osteophyte width removed with sufficient force to obtain a firm end point. In the present study, mean femoral osteophyte size in the medial compartment was 4.4 ± 1.7 mm. According to Pottenger et al.'s study,20) an increase in mean varus-valgus angle of about 1.62° (3.6 × 0.45) would have been expected during the present study. Also, as we measured only the valgus angle, we would have expected a valgus angle change of < 1.62°, a relatively small amount. These findings suggest that if osteophytes do not become large enough to affect joint stability, the effect of osteophyte size on preoperative VSA is minimal.
Varus alignment of the articular surface of the proximal tibia (proximal tibia vara) has been noted in many cases of medial compartment OA.21) Verdonk et al.1) suggested that preoperative alignment and amount of proximal tibia vara, the latter of which was estimated using MTA, are important preoperative indicators of the medial release technique. In the present study, preoperative MTA was found to show a weak positive correlation with preoperative VSA. We had speculated that varus deformity with proximal tibia vara would be corrected without excessive medial release in cases with a small preoperative VSA for the following reasons: the mechanical axis of the tibia would deviate to a similar extent with proximal tibia vara severity; and this deviation would be reflected by VSA without severe medial soft tissue contracture. However, proximal tibia vara was found to have the opposite effect on the amount of medial release. A highly significant negative correlation was obtained between preoperative MAA and MTA, which meant that MTA was correlated with severity of varus deformity. In other words, if MTA becomes small (proximal tibia vara), MAA becomes large (severe varus deformity). Furthermore, osteoarthritic knees tend to develop ligament pseudolaxity in the involved compartment, which appears to be due to a loss of cartilage and bone on the joint surface. Furthermore, ligaments of the knee are capable of adapting to altered loads by changing their material properties and dimensions,22-24) and the severity of medial soft tissue contracture can be altered by the severity of varus deformity. This is why extensive medial release is more frequent in cases with a smaller MTA. We are of the opinion that preoperative MAA and MTA be considered with preoperative VSA, when determining the amount of medial release required to correct varus deformity during TKA.
In addition, VSA can change in accord with medial soft tissue contracture severity and femoral and tibial anatomic morphologies, which can change the mechanical axis of the knee. Cooke et al.25) suggested that the prevalence of patient with medial osteoarthritis showing excessive valgus angulation of the femoral joint surface with proximal tibial vara was 11.5%. This configuration causes a downward and medial inclination of the articular surfaces in the coronal plane and lateral thrust of proximal tibia, which causes medial shifting of load-bearing axis. This may overestimate varus deformity, and if MFA are excessively large (valgus angulation of distal femur), varus deformity of the knee may not be severe, despite the small MTA. However, we could not evaluate cases with excessively large MFA.
This study has several limitations. First, all study subjects were patients who visited our hospital with symptoms and structural changes typical of knee OA, and thus, our findings are not sufficient to establish a general finding of knee OA. Also, the patients were not all severe varus deformity patients. Second, we retrospectively reviewed preoperative radiographs, and thus, radiographs were not precisely controlled. It is possible that slight variability of knee positioning and rotation influenced assessments of the size and alignment of osteophytes. Finally, a two-dimensional method was used to measure osteophyte size, and thus, it was difficult to differentiate osteophytes affecting medial compartment in extension from those that affected it in flexion. We thought that osteophytes affecting the medial compartment in extension would be associated with preoperative VSA. However, as far as we are aware, only one method for measuring osteophyte size using radiographs has been described in the literature.10) To reduce potential bias caused by osteophyte size measurements, we tried to measure osteophytes near the distal articular surface of the femur.
Preoperative varus deformity (measured by preoperative MAA) and proximal tibial vara (measured by preoperative MTA) were factors correlated with reducibility of varus deformity (measured by preoperative VSA). The clinical parameters (age, ROM, duration of pain, and BMI) and other radiologic parameters (osteophyte size, severity of OA, and angulation of distal femoral joint surface) were not significantly correlated with reducibility of varus deformity.




 XML Download
XML Download