

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Malignant melanoma is a class of malignant tumors derived from neural crest cells. Its rate of occurrence is low, accounting for 1%-3% of all malignant tumors. Cutaneous melanoma is the most common cause of mortality amongst skin cancers in Caucasian populations1,2) and incidence rates per 100,000 patient years vary between 21.9 in the United States to 55.9 in Australian males.3) In contrast, the incidence of melanoma in Asia is significantly lower with incidence rates of 0.2 to 0.5 per 100,000 patient years.4,5) However, in Asian populations, there are only a few published reports since the incidence is much lower.6-8) In comparison to the cutaneous melanomas arising in Caucasians, they occur more commonly in unusual sites (e.g., hands and feet) in Asians in the form of acral melanomas.3-6) Due to the rarity of their occurrences and acral presentations, diagnosis is often delayed, resulting in more advanced stages of disease at presentation.9) Therefore, advanced stage melanomas on the extremities frequently require wide surgical excision, such as amputation. It is generally believed that melanomas arising in acral locations are initially diagnosed at a more advanced stage and that this may account for its grave prognosis.9) To confirm this, we reviewed our experience in the management of advanced stage melanoma, especially melanoma occurring on the hands and feet, after wide surgical excision, including amputation.
METHODS
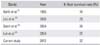
The cases were collected from our melanoma database, and 30 patients who were treated from January 2001 to December 2010 were retrospectively reviewed. Medical records were reviewed for demographics, clinical and pathological information, immediate as well as remote postoperative events and outcomes, with a minimal follow-up of 2 years or death. All patients were advanced stage (American Joint Committee on Cancer [AJCC] stage II and III) melanoma patients, and for the operative treatment, we performed wide marginal surgery, which sometimes involved removal of the bone and surrounding tissue. And without considering the stage of the melanoma, we routinely performed sentinel lymph node dissection in all patients. Therefore, we performed amputation with lymph node dissection for all patients who had melanoma of AJCC stage III (Table 1). After the surgery, we monitored patients for recurrence and metastasis every 3 months for the first 2 years and then gradually lengthened the interval between visits to yearly by the fifth year if no relapse of disease was observed. Patients underwent history, physical examination, chest radiography, and radiography of the affected region at each visit. Computed tomography, magnetic resonance imaging, and whole-body bone scans were obtained selectively, depending on whether there was evidence from the history, physical examination, and radiographs to warrant further study. Data extracted included early diagnosis, sex, location of the tumor (hand or foot), and for the clinical evaluation, we used the AJCC classification.10) Also, patient's mortality, follow-up duration, the date of the first operation, and metastasis to the sentinel lymph node were assessed. Data on survival (from the date of diagnosis to the date of last follow-up or death) for the survival analysis was acquired from our database.
For the statistical analysis, the Kaplan-Meier product was used to estimate curves for survival rate, and the log-rank test was used to evaluate differences between the survival curves. Patients who were lost to follow-up or who were alive at the time of the last follow-up were censored at the date of their last follow-up. A p-value < 0.05 was considered statistically significant. Univariate t-test analysis was used to calculate the relative risk of each parameter. We used the SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) to perform statistical calculations and calculated confidence intervals of 95% for the statistical parameters.
RESULTS
Patient Characteristics
Table 1 summarizes the clinical and pathologic data for our patients. Eighteen of the 30 patients (60%) were men and 12 patients (40%) were women, for a male-to-female ratio of 1.5:1. Most were diagnosed while in the sixth or seventh decade of life, with a mean age of 58.7 years (range, 35 to 78 years). All of the patients had AJCC stage II or III disease at initial examination, and lesions were located predominantly on the sole and thumb (Fig. 1).
Thirty patients who were diagnosed with high-grade malignant melanoma, underwent amputation of the tumor-involving extremity. The overall survival of patients after amputation of the malignant melanoma was 93% at 1 year, 76% at 2 years, and 67% at 5 years (Fig. 2). Fourteen of 30 patients were alive without disease, and six patients were dead with the disease at the end of the study (Table 2).
Overall Survival and Prognostic Factors
On the univariate analysis, diagnosis when over 70 years of age, tumor located on the lower extremity, and postoperative lymph node metastasis were found to predict poorer survival; and this result was statistically significant (p < 0.05) (Table 3). And on the Kaplan-Meier analysis, patient's gender and location of the tumor did not affect long term survival, whereas age at diagnosis, AJCC stage, and postoperative lymph node metastasis did impact the survival (p < 0.05) (Table 4).
The overall survival curve was plotted according to age, sex, location, AJCC stage, and postoperative lymph node metastasis (Fig. 3). And as mentioned above, there were significant differences in early diagnosis, AJCC stage, and postoperative lymph node metastasis of malignant melanoma (p < 0.05). We also found amputation with aggressive lymph node dissection improved the 5-year overall survival of AJCC stage III patients, with a survival rate of up to 32.1%.
DISCUSSION
Malignant melanoma is a relatively rare occurrence in the Asian population compared to fair-skinned populations. Limited data are available on skin cancer in Asians, including information on the prevalence rates of malignant melanoma in different Asian populations.11) In Korea, the incidence of malignant melanoma increased from 1.02% of all skin malignancies in the 1980s to 15.6% in the 1990s.12,13) The mean age of diagnosis of melanoma was 58.7 years in our study, which was similar to other studies.14) In Asian populations, malignant melanoma tends to occur 1.5 times more often in males than females, as in our study.14) Unlike other studies, all of our patients were consulted from the dermatologic department with more than AJCC stage II, which is advanced stage malignant melaoma. The difficulty in making the diagnosis of these malignant melanomas and the subsequent delay in proper treatment are factors likely to contribute to the preponderance of advanced lesions seen at the initial presentation.15-17) In this study, all of the patients presented with either AJCC stage II or III, and all cases were more than 1.5 mm thick. These factors (stage, thickness, and level of invasion) are important prognostic parameters in patients with advanced stage melanoma.18-21) After diagnosis of the melanoma, the affected digit must be amputated promptly. Confirming a previous report,17) most studies of subungual melanoma have used amputation with or without lymph node dissection, yielding 5-year survival rates of 16% to 32%,22,23) whereas others using amputation with lymph node dissection or regional limb perfusion have reported 5-year survival rates of 25% to 32%, with minimal morbidity and no mortality.24,25) In addition to amputation, most patients underwent lymph node dissection and regional limb perfusion. Although the use of these treatment modalities did not affect patient survival, perfusion may reduce the incidence of local disease recurrence. There is still controversy about the significance of the anatomical site of origin in prognosis. In our study, 85% of the melanomas were located on the acral area (palm, sole, and subungal area). However, when compared with melanomas arising in other locations, sex and thickness of tumor were not significantly different. According to the location of the tumor, our institution performed wide marginal resection of the tumor, that is, amputation. The principle treatment for primary malignant melanoma is wide marginal excision. But, treatment of melanomas on the hands and feet is particularly challenging for surgeons due to the functional uses of these body parts and the difficulty of obtaining the conventionally recommended margins. However, in cases of advanced stage melanoma as in our studies, amputation is usually required due to the paucity of soft tissue between the tumor and the bone. Therefore, although amputation is not commonly recommended in general, it should be the first recommendation in cases of advanced stage melanomas that have insufficient safety margins. Balch et al.26) reported 5-year survival rates of 13% to 37% in patients who showed lymph node metastasis at the time of diagnosis. Although, in our study, patients who were diagnosed as AJCC stage III showed a poorer survival rate than stage II patients, with aggressive lymph node dissection during the amputation, we found an improved survival rate of AJCC stage III patients of up to 32.1%, higher than in other reports (Table 5).27-30)
In Korean melanoma patients, for the treatment of high grade melanomas on the extremities after amputation, early diagnosis and postoperative follow-up for evaluation of lymph node metastasis are critical factors for long term survival. By performing lymph node dissection during amputation, we may improve the survival rate in advanced stage melanoma patients.






 XML Download
XML Download