

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Sexual activity is an integral part of the quality of life and affects it.1,2) A dysfunction in sexual activity is known to be strongly associated with physical and emotional dissatisfaction and depression.3)
Studies on sexual activity after total hip replacement have reported that the adverse effects of arthritis of the hip joint on sexual activity are ameliorated after total hip replacement (THR).4-6) These studies have also emphasized the role of physicians in educating the patients on sexual activity after THR.
However, the concerns of patients as related to sexual activity after THR have not been well studied, and thus, we do not have a well-established protocol on how to educate patients. Furthermore, most reports on sexual activity after THR are as issued in Western countries, and Asian patients are expected to behave in a different fashion.7)
This study aimed to determine: (1) what are the concerns of patients related to sexual activity after THR? (2) What are the changes in sexual activity after THR in Korean patients?
METHODS
This study was conducted using a questionnaire administered during a face-to-face interview. The interviews were performed from November 2007 to January 2009 at an outpatient clinic. The study inclusion criteria were a married status, an age of ≤ 65 years at the time of the study and primary THR of more than 6 months before the study commencement. Patients who did not have sexual activities during the previous year were excluded. The patients who had dislocation, infection and stiffness after THR were also excluded. The surgery was performed by a single surgeon using a posterolateral approach. The surgical indication for THR was a painful hip joint, with the radiological evidence of hip-joint destruction which failed to respond to conservative treatment. Five hundred and twelve patients satisfied the inclusion and exclusion criteria. Of these patients, 343 refused to participate, and 105 patients had no sexual relations for 1 year after THR. Finally, 64 patients participated in this study. The demographic characteristics of the patients are summarized in Table 1.
The questionnaire was constructed using the questions devised by Currey5) and Meyer et al.,8) with additional questions designed to investigate the concerns associated with sexual activity. The open questionnaire was composed of four questions: (1) What issue troubles you the most during sexual activity? (Appendix 1) (2) What concerns you the most about sexual activity? (3) How did you get information related to sexual activity after THR? and (4) If you did not discuss sexual activity with your physician after THR, what was the reason?
A pilot study was performed at an outpatient clinic on twenty patients. As too many questions reduced the quality of responses, we restricted the total number of questions to twenty and focused on questions that addressed the sexual activity concerns. Male patients were interviewed by a male fellow, and female patients by one experienced female physical assistant, who had supervised patient interviews at our department for six years. All interviews were performed during a routine follow-up visit.
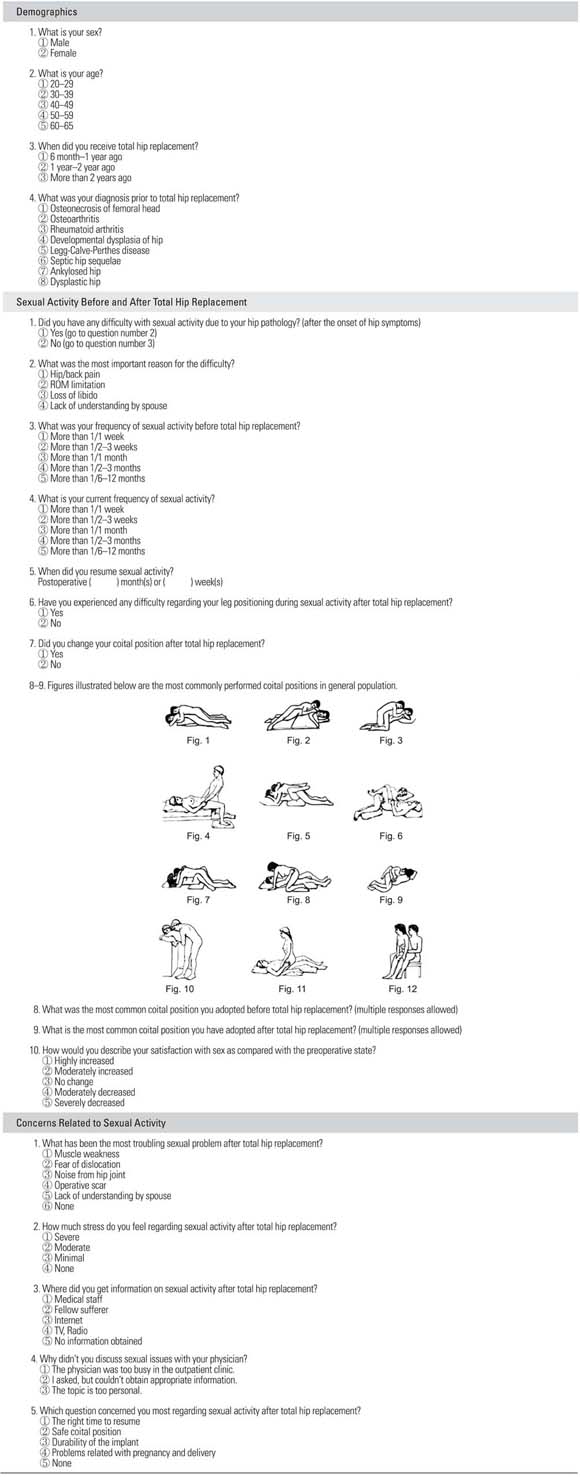
The final questionnaire was composed of three parts, which addressed demographic factors, sexual activity before and after THR, and concerns related to sexual activity after THR. Demographic factors included sex, age, time period after THR, and diagnosis. Questions on concerns related to sexual activity after THR addressed: the biggest problem during sexual activity; stress level related to sexual activity; source of information on sexual activity; reasons for not communicating with a doctor at the outpatient clinic on sexual activity; and the question of greatest interest. Questions on sexual activity before and after THR addressed: whether hip pathology before THR adversely affected sexual activity (and if yes, what the most significant reason was); the frequencies of sexual activity pre- and postoperatively; the time of resumption of sexual activity after THR; difficulty with leg positioning during sexual activity after THR; changes in sexual position after THR; the most common coital position before and after THR; and changes in satisfaction rate after THR. The twelve examples of the most common coital positions were taken from an article by Dahm et al.9) (Appendix 1).
The Student t-test was used to compare the time to the resumption of sexual activity. Frequencies were calculated for all categorical/ordinal variables. Categorical variables, such as sex, difficulty with leg positioning and change in sexual position, were compared using the chi-squared test. To examine the relation between stress level and satisfaction rate, both were collapsed into two categories: stress level was dichotomized as moderate/severe or minimal/none; and satisfaction rate as increased or as no change/decreased group. For these, comparisons were made using with Fisher exact test. Statistical analysis was performed using SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was accepted for p-values of < 0.05.
RESULTS
Preoperatively 34 patients (53.1%) had sexual activity difficulties due to the hip pathology, and there were no differences for the sexes. Of those patients with preoperative difficulties, the most common reason given was a limitation of motion (61.8%), followed by a hip/back pain (17.6%) (Table 2).
The most troubling problem during sexual activity was the fear of dislocation, followed by weak muscle power (Table 3). Fifty-one patients (79.7%) were not able to obtain information on sexual activity after THR. Of the thirteen patients who managed to obtain information, the internet was the most common source (8 patients, 61.5%), followed by medical staff (3 patients, 23.1%). Of the 61 patients who did not consult with a physician, 55 patients (90.2%) responded that the topic was too personal to discuss, and 6 patients (9.8%) cited an unsuitable environment in outpatient clinics. The question that most patients wanted answered concerned the safety of coital positions (39 patients, 60.9%), and the second most common question concerned the time of resumption.
Twenty-five patients (39.1%) had difficulties with leg positioning during sexual activity after THR, and female patients had more difficulties with the leg positioning (p = 0.045). Twenty-six patients (40.6%) changed preferred coital position after THR, and the patients with leg-position difficulties changed positions more frequently (p < 0.01). No difference was observed between the sexes. Preoperatively, the most common coital positions were the same for both sexes (No. 5, 7, 8, 11, 4 in descending order). However, postoperative coital positions differed between the sexes. For male patients, the most common five positions postoperatively were No. 5, 7, 8, 10, and 11, but in female patients, they were No. 7, 8, 3, 4, and 5 (both in descending order).
Most patients (68.9%) showed no changes in the frequency of sexual activity after THR. Three patients (4.5%) reported an increase, and seventeen (26.6%) a decrease in frequency after THR. Mean time to the resumption of sexual activity was 6.19 months (range, 3 weeks to 48 months), and the median time was 3 months. There was no difference between the sexes (Fig. 1).
Satisfaction pre- to postoperative did not change for most patients (68.8%): 15 patients (23.4%) reported greater satisfaction, and 5 patients (7.9%) less satisfaction. When stress level and satisfaction rate were divided into two categories (stress level into severe/moderate or minimal/none; and satisfaction rate into no change/decreased or increased), the minimal/no stress groups were found to have greater satisfaction postoperative (p = 0.03).
DISCUSSION
Dysfunction in sexual activity is known to be strongly associated with physical and emotional dissatisfaction and depression.3) Total hip replacement is known to ameliorate the adverse effects of arthritis of the hip joint in sexual activity.4-6) However, concerns of patients related to sexual activity after THR have not been well studied, and thus, we are not well placed to decide on how to educate the patients. This study was undertaken to document the changes in sexual activity before and after THR in Korean patients, and to investigate patient concerns related to sexual activity after THR.
This article has some limitations which are inherent in this type of study. First, the retrospective nature of this study means it is limited by the patient recall. Second, personal face-to-face interviews may distort information, especially when the questions address sensitive issues.10,11) Third, due to the low response rate, our study population was too small to undertake a deeper statistical analysis or to comment on clinical significance. Nevertheless, we tried to understand the patients' concerns regarding sexual activity after THR and how THR affected sexual activity satisfaction and frequency. In view of the complex nature of sexual activity,12) relieving patient concerns may be one of the easiest ways of improving satisfaction, and eventually, the quality of life. Fourth, we did not evaluate correlation between changes in sexual activity and causative diseases.
Preoperatively, 53.1% of patients had difficulties due to hip pathology, which was the most common difficulty. Median time to resumption of sexual activity was 3 months, and most patients showed no increase in the frequency of sexual activity after THR. These responses show similar patterns to those found in the Western studies. Reported rates of sexual difficulty attributable to hip pathology range from 46% to 67%,5,8,13) which is similar to that found in the present study. We found that limitation of motion was the most common reason for sexual difficulty, which also agreed with previous studies.5,8,13) However, the frequency of sexual intercourse was increased for 3 patients only (4.5%), which was substantially lower than that reported in the West.8,13,14)
The most common fear during sexual activity was that of dislocation, and the issue of greatest concern was the fear of dislocation during sexual activity. Furthermore, patients with higher stress levels were found to have lower satisfaction rates. The unresolved concerns regarding medical treatments are known to be associated with reduced patient satisfaction, lower adherence and possibly poorer health-related outcomes.15-17) Moreover, it has been established that not seeking help for sexual difficulties has a negative impact on the quality of life.3,18) This study shows that a higher stress level is associated with poorer satisfaction, with the most common concern during sexual intercourse being the fear of dislocation. It also shows that the question patients wanted to ask concerns safe positions during intercourse. These findings indicate that educating patients regarding safe positions during sexual intercourse is likely to lower stress levels and improve satisfaction rates.
Most patients were unable to obtain information regarding sexual activity after THR, and did not consult with a physician due to the personal nature of the topic. The internet was the most common source of information among those who managed to obtain information on sexual activity. Generally speaking, most patients are reticent about discussing sexual concerns with physicians,1,19) which means it is difficult to determine what the concerns are. As shown in the present study, most patients did not discuss the issue with physicians, because for most, it was deemed too personal, and obtained the information from the internet instead. However, studies on the quality of medical information provided by the internet show that it is often misleading and of poor quality, which means that patients may be provided with incorrect information.20-23) Consequently, we believe that education on safe positions during sexual intercourse must be undertaken regardless of whether advice is requested for an improvement of sexual relations and patient safety.
In 39.1% of patients were shown difficulties with leg positioning after THR, and these patients were more likely to change the coital position. Of the twelve illustrated coital positions, males tended to adopt the same position before and after THR, whereas females were more inclined to make a change. The coital position changes after THR of the present study were concordant with those found by Laffosse et al.;14) that is, there were no change in male patients, but some changes in female patients. When compared with the coital positions recommended by the American Association of Hip and Knee Surgery,9) most male patients adopted the recommended positions (No. 5, 7, 8, 10, and 11), whereas female patients tended to prefer non-recommended positions. While the recommended positions for female patients were No. 1, 4, and 10, the actual preferred positions were No. 7, 8, 3, 4, and 5 in order of preference. In addition, female patients complained more frequently of the leg-positioning difficulty. These findings indicate that further education on safe coital positions is required for female patients.
Sexual activity is an important dimension of quality of life. Although THR patients do not often communicate with physicians concerning sexual activity, they have real concerns. Providing the patients with relevant information is likely to alleviate their concerns and enhance satisfaction. Furthermore, this advice is more important for female patients, as they have shown a tendency to adopt the non-recommended coital positions.




 XML Download
XML Download