

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Recently, various methods for anterior cruciate ligament (ACL) reconstruction have emerged, reflecting the development of novel biomechanical knowledge and surgical techniques.1-3) Most studies on ACL reconstruction have focused on how the characteristics of natural ACL can be restored. The femoral tunnel position in ACL reconstruction determines biomechanical property of the graft and affects knee function. Although the isometric point of the femoral side for single bundle ACL reconstruction had been used as the standard method, its potential to cause rotational instability has replaced the anatomical footprint method as the preferred tool.
Techniques for creating anatomical femoral footprint in single bundle reconstruction have been reported, such as the trans-anteromedial (trans-AM) portal technique and the outside-in technique. However, disadvantages such as insufficient femoral tunnel length, posterior wall breakage and a bent graft will limit the use of trans-AM portal technique.4) Similarly, acute femoral tunnel angle, inadequate femoral fixation, and additional lateral skin incisions upon surgery are major hindrances for the use of the outside-in technique.5) In this paper, we describe an unusual approach to the traditional transtibial method to fix the anatomical femoral tunnel. The traditional transtibial method, while overcoming the disadvantages of the former two methods, has an advantage of relative easy and familiar technique for most surgeons and allows early rehabilitation by initial strong fixation. However, a short and shallow tibial tunnel can be formed.6,7)
The authors adapted this transtibial technique to make an anatomical femoral tunnel and evaluated the tunnel position with 3-dimensional computed tomography (3D-CT) and plain radiography. Our hypothesis was this modified transtibial technique that we have developed could create a functional anatomical femoral tunnel in ACL reconstruction.
METHODS
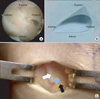
Between December 2010 and October 2011, 98 patients who were diagnosed with isolated ACL ruptures underwent primary ACL reconstruction using single bundle method with modified transtibial technique. Informed consent was obtained from all patients prior to receiving 3D-CT and radiograph for analyzing the femoral tunnel position after the operation. The patient pool consisted of 81 men and 17 women with a mean age of 27.3 years (range, 15 to 60 years). The femoral tunnel angle was evaluated from the plain radiograph (Fig. 1C) by two orthopedic surgeons on two separate occasions at an interval of 2 weeks to assess the interobserver and intraobserver reliability.
The quadrant method used to measure the postoperative femoral tunnel position by 3D-CT is as follows: 1) A true lateral view cutting at the middle of the intercondylar notch of the proximal femur by 3D-CT was attained through the picture of archiving and communication systems (PACS, Marotech, Seoul, Korea) (Fig. 1A). 2) The image was enclosed with a rectangular measurement frame that was either parallel or perpendicular to the Blumensaat line on Power Point ver. 2007 (Microsoft Co., Redmond, WA, USA) as shown in Fig. 1B. t calculated the deep to shallow distances from the center of the femoral tunnel parallel to the Blumensaat line, and h calculated the high to low distances perpendicular to the Blumensaat line. In addition, the anatomical femoral attachment site of ACL was shown on Table 1 using the previous quadrant method.
Surgical Techniques
After thorough arthroscopic evaluations of the ACL, a 3 cm longitudinal skin incision at 2 cm medial to the tibial tuberosity was made. A single semitendinosus tendon was harvested as usual. The graft was cut in half and folded into half to produce a quadruple semitendinous graft. If the harvested graft was shorter than 24 cm, a quadruple semitendinosus/gracilis graft was prepared by harvesting both the semitendinosus tendon and the gracilis tendon.
The intercondylar ridge of the lateral femoral condyle, and the bifurcate ridge that divides the AM bundle and the posterolateral (PL) bundle were confirmed by removing the soft tissues at the femoral insertion of ACL. The remaining ACL fibers were generally preserved. A bony mark at the anatomic center of ACL footprint (just posterior to the bifurcate ridge and center of anteroposterior [AP] width of footprint) was made by passing a microfracture awl through the anteromedial portal as in Fig. 2A. This center was deepened and widened to allow space for the guided pin through the tibial tunnel. Since the anatomical femoral tunnel is prepared by the trans-AM portal, the transtibial guide pin tends to be located more to the anterior and proximal position of anatomic center than anticipated. The 'triangular, funnel-shaped bony trough' was employed to slip the eccentrically positioned guide into the anticipated anatomic center, which is part of our modified transtibial technique (Fig. 2A, B).
The starting point of the tibial edge/periphery was superior to the pes anserinus and the anterior margin of medial collateral ligament (MCL) (Fig. 2C). The intra-articular site is positioned immediately lateral to the medial tibial spine and the extension of the inner margin of anterior horn of lateral meniscus. The reference point of tibial tunnel is a little posterior region of the ACL footprint. The angle of the ACL guide (Linvatec, Largo, FL, USA) was set at 47.5°. The tibial tunnel was created using a reamer with diameter 1 mm smaller than the prepared ACL graft.
With a free hand technique, a guide pin was passed through the tibial tunnel towards the bony trough. Generally, the guide pin was located distal and anterior to the anatomical center, and extension of the knee nudged the guide pin towards the proximal and posterior region of the anatomic center, but was being bent at the intra-articular orifice of the tibial tunnel (Fig. 3). Femoral reaming was performed with knee flexion which reduces the chances of blowing out the posterior wall and increases the femoral tunnel length. When the reamer passes over the bending portion of the guide pin, the knee should be extended. After passing through the bending point, the knee could also be flexed.
After the graft passage, femoral fixation was done with Endobutton and Bio-Cross Pin (RigidFix System, Mitek, Johnson & Johnson, Norwood, MA, USA). If femoral tunnel was short, the graft was press fitted with only Endobutton. The graft was tensioned and fixed to the tibia by placing the HA screw (Bioscrew poly L-lactic acid, Linvatec
Linvatec).
Postoperative Rehabilitation
All patients underwent the same standardized rehabilitation protocol as a home-based exercise. We regularly performed follow-ups on the patients in the out-patient clinic and established a protocol for rehabilitation. The patients were allowed full weight bearings with unlocked braces 2 weeks after surgery. Partial weight bearing with crutches for 6 weeks was mandated for patients who underwent meniscal repairs. The treatment purpose of the patients was to gain a full range of motions at 2 to 6 weeks after surgery. A perturbation training program began at 6 weeks after surgery. Running and side-cutting activities were allowed at 3 months, with a return to sports activities at 6 months after surgery.
RESULTS
The position of the femoral tunnel was measured using the quadrant method by 3D-CT,8) where t was 32.94% ± 5.16%, and h was 41.89% ± 5.58% (Fig. 4). These values were more distal and middle as compared with the previous data (mean t, 29.85%; h, 33.2%) measured by quadrant method using cadaveric knees for validating anatomical ACL footprints (p < 0.05).9,10) The interobserver intraclass correlation coefficients (ICCs) were 0.766 and 0.793, whereas the intraobserver ICCs were 0.875 and 0.893. The femoral tunnel angle on the AP view was 50.43° ± 7.04°, for which the interobserver ICCs were 0.783 and 0.795, and the intraobserver ICCs were 0.911 and 0.923.
On the process of optimizing this modified transtibial technique, mishaps such as breakage of the bended wire occurred on 3 occasions as the reamer passed through the tibial tunnel, and a shallow tibial tunnel was formed on another occasion, which all occurred during the initial series. However, as the examiners became more experienced in executing this modified technique and when the safe zone of the bone stock was adjusted to the entry point of the tibia, these complications were avoided.
DISCUSSION
The purpose of this study is to describe a single bundle ACL reconstruction performed with modified transtibial technique for positioning the femoral tunnel to anatomical footprint.
The femoral tunnel location was being evaluated with 3D-CT scan reconstructions with the quadrant method as described by Bernard et al.,8) and the results of these scans were compared with those derived from arthroscopic identification. The results of this study showed that the t-value was 32.94% ± 5.16%, and the h-value was 41.89% ± 5.58%. Abebe et al.11) and Kaseta et al.12) reported that the femoral tunnels were placed "deeper or more proximal" and "higher or more anterior" than the native ACL insertions of the femur when the transtibial technique was used, which could result in increased laxity of the graft. Contrary to these results, the femoral tunnel in this study was located "shallower or more distal" and "lower or more posterior" than the mean value from multiple measurements of the anatomical ACL footprints in cadaveric knees (t, 29.85%; h, 33.2%) from previous studies that also used the quadrant method for calculation. The mean values of the femoral tunnel created by the authors were placed between the AM and PL bundle position, which were calculated as described by Kopf et al.13) and Tsukada et al.10) Rue et al.6) reported that a laterally-oriented transtibial drilling femoral tunnel effectively overlapped approximately half the AM bundle and half the PL bundle. Miller et al.14) proved that the intra-articular aperture of the femoral tunnel in all cases formed an ellipse, with the long and short axis averaging 13.9 ± 1.6 mm and 9.4 ± 0.8 mm in the trans-AM method, and 12.1 ± 0.8 mm and 10.6 ± 0.6 mm respectively in the transtibial group. Accordingly, if the center of the femoral tunnel is relatively "distal" and "posterior," the ellipse-shaped tunnel would allow the incorporation of original portions of the AM and PL bundles leading to a more anatomical reconstruction. Hence, this modified transtibial technique has advantages over the traditional technique (t, 37.2% ± 5.5%; h, 11.3% ± 6.6%) for being closer to its anatomical location.10,13) Ferretti et al.15) reported the presence of a lateral intercondylar ridge in all patients who underwent ACL reconstruction and the bifurcate ridge in 82% of 60 knees. van Eck et al.16) described 88% and 48% of these landmarks, respectively for their patients at arthroscopy. However, to arthroscopically identify these landmarks on the medial wall of the lateral femoral condyle is difficult. Therefore, postoperative 3D-CT scans were used to validate whether this modified technique can reproducibly be used for the placement of the anatomic femoral tunnel.
Our angle of the femoral tunnel in the coronal plane was on average 50.43° ± 7.04°, when viewed by AP radiography, and it was lower than the results (61.7° ± 5.5°, 58.8° ± 8.3°) from previous transtibial techniques, even when compared with the anteromedial portal technique (55.9° ± 4.7°, 50.9° ± 8.3°), which were measured by Chang et al.17) and Dargel et al.18) In addition, Bedi et al.4) reported that the coronal angles of the oblique femoral tunnels from either the transtibial or the trans AM portal techniques were 54.1° ± 7.17° and 45.9° ± 6.9°, respectively. Therefore, the rate of the posterior wall blowout was 50% with the latter technique. Thus, not only is the modified transtibial technique more reproducible, but it is also safer when such complications of the AM portal technique is taken into consideration. There was no significant posterior wall blowout in our case series.
The entrance of the tibial tunnel is essential for the placement of the anatomic femoral tunnel when using the transtibial technique for ACL reconstruction, especially if we want to prevent graft failures.19) Recent studies have tried to accurately drill the tibial tunnel in relation to the native ACL footprint of the femur, but without success.20,21) However, Heming et al.7) reported the plausibility of the anatomical footprint using the transtibial technique, but commented that the starting point should be closer to the joint line, and the tibial tunnel length must be shortened for an accurately positioned footprint. Arnold et al.22) attempted to produce anatomical tunnels by transtibial drilling just proximal to the pes anserinus and ventral to the MCL, but in their case, the guide pin was projected too high in the notch and missed the femoral insertion. In this study, the authors followed Arnold's method to avoid creating shallow tibial tunnels, and furthermore, used a new modified method to prevent over-projecting the guide pin in the notch into a non-anatomical position.
There are some advantages of this modified transtibial technique in which the femoral tunnel is drilled appropriately through the tibial tunnel. First, it is similar to the conventional method and easily replicated by surgeons who are familiar with the transtibial technique. Second, it is possible to create the femoral tunnel in an anatomic position through a relatively longer and deeper tibial tunnel with only a few additional and simple techniques; triangular, funnel-shaped bony trough and by changing knee flexion angles during femoral tunneling. Third, it permits early rehabilitation through firm graft fixation resulting from tunnel length-graft length matching.
The limitations of the study may be that the authors used the mean values of the native ACL insertions derived from multiple previous studies for comparison. Although the methods used in this paper are the same as those in previous studies, mean variations in the experimental instruments do not reflect the differences that arise, and, are therefore, a crude averaging of values. In addition, the ICC was lower for the interobserver correlation coefficient in two observers, which may reflect the difficulty of selecting the true lateral view on the magnetic resonance imaging sagittal image, and measures the center of the femoral tunnel (forming an ellipse interobservers). Finally, there was a lack of full considerations for the length of the femoral tunnel and the characteristics of the tibial tunnel. Further studies to overcome these limitations are required, and essential evaluations of clinical outcomes for modified transtibial technique are necessary to prove its superiority over the traditional techniques.
In conclusions, our modified transtibial technique is anticipated to provide a true anatomical placement of the femoral tunnel during ACL reconstruction than the previous traditional transtibial techniques.




 XML Download
XML Download