

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Fractures are common orthopaedic problems in children and adolescents, which require urgent or emergency management in most cases. These unpredictable emergencies can place a significant burden on medical resources, and often results in the excessive workload of medical personnel and a shortage of hospital rooms for admission. This may be a systematic factor in the delivery of inappropriate medical care.
Previous studies have reported the incidence of specific fractures differs according to age, season, weather, and day of the week, etc.1-17) These studies provide information on the risk factors for fractures, and possible preventive measures for fractures. On the other hand, most studies have been confined to specific fractures, specific age groups and specific hospitals,1,2,4,7,9,11,13-18) and there is insufficient population-based data given by these studies, particularly data covering the nationwide population.
This study examined the incidence of several pediatric and adolescent orthopaedic fractures including clavicle, distal humerus, both forearm bone, distal radius, femoral shaft, and tibial shaft fractures based on nationwide population data, as well as the incidence patterns according to seasonal variations and age groups.
METHODS
The institutional review board at our hospital waived approval for this study because it did not involve human subjects as materials.
Study Population
The data of this study originated from the nationwide population of South Korea, which has a total population of 48,219,000 as of 2009. Approximately 10 million children and adolescents aged 18 years and under who were enrolled in the national health insurance system comprised the study population.
Data Collection
Data on the number of pediatric and adolescent patients who utilized medical services due to fractures were retrieved from the Health Insurance Review and Assessment (HIRA) service. This institute reviews the suitability of payments from the national health insurance scheme to medical institutes, and also mediates in disputes between producers and consumers of medical services, assesses the adequacy of medical practice, and assists in the development of government health policy in South Korea.
The data obtained from the HIRA contained the monthly number of pediatric and adolescent patients between 2005 and 2009 according to four age groups (0-4 years, 5-9 years, 10-14 years, and 15-18 years) with diagnostic codes of S42.0, S42.4, S52.4, S52.5, S72.3, and S82.2 (in International Classification of Diseases 10), which represent clavicle fractures, fractures of the distal humerus, both forearm bone fractures, distal radius fractures, femoral shaft fractures and tibial shaft fractures.
Incidences of Fractures and Seasonal Variation
The annual incidence of each fracture was calculated by dividing the total number of children and adolescents that were enrolled in the national insurance system by the total annual number of children and adolescent patients with the fracture. The incidences were represented as the incidence per 10,000 per year with 95% confidence intervals (CI). The seasonal incidences were also presented per 10,000 per year. Incidence variation was calculated by dividing the highest incidence by the lowest incidence.
Statistical Methods
No specific statistical analysis was used other than descriptive statistical analysis because this study included the whole population. The distribution of fracture onset within the four seasons was tested for homogeneity in the total fracture population for each fracture type, using the chisquare test for goodness of fit with Bonferroni's correction.
RESULTS
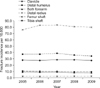
The annual incidence of clavicle fractures, distal humerus fractures, both forearm bone fractures, distal radius fractures, femoral shaft fractures and tibial shaft fractures were 27.5 (95% CI, 27.2 to 27.8), 34.6 (95% CI, 34.2 to 34.9), 7.7 (95% CI, 7.5 to 7.9), 80.1 (95% CI, 79.6 to 80.6), 2.5 (95% CI, 2.4 to 2.6), 9.6 (95% CI, 9.4 to 9.7) per 10,000 per year in 2009, respectively. Both forearm bone and tibial shaft fractures showed a slightly decreasing trend and femoral shaft fractures showed a slightly increasing trend between 2005 and 2009 (Fig. 1).
In 2009, clavicle fractures showed a peak incidence of 46.0 (95% CI, 45.1 to 46.9) in age group 0-4 years and a decreasing incidence with age. Distal humerus fractures showed peak incidence of 71.0 (95% CI, 70.0 to 72.0) in the 5-9 year age group, followed by the 0-4 year age group. The peak incidence of both forearm bone fractures was 11.1 (95% CI, 10.8 to 11.5) in the 10-14 year age group, showing a similar incidence of 10.7 (95% CI, 10.3 to 11.1) in the 5-9 year age group. Distal radius fractures showed the greatest variation according to the age group: 148.1 (95% CI, 146.8 to 149.4) in the 10-14 year age group and 19.0 (95% CI, 18.5 to 19.6) in the 0-4 year age group. Femoral shaft fractures showed the least variation according to age groups; the incidence was 1.9 (95% CI, 1.8 to 2.1) in the 10-14 year age group and 3.6 (95% CI, 3.3 to 3.8) in the 15-18 year age group. Tibial shaft fractures showed a decreasing incidence with increasing age; incidence was 13.5 (95% CI, 13.0 to 14.0) in the 0-4 year age group and 5.7 (95% CI, 5.5 to 6.0) in the 15-18 year age group (Fig. 2).
In terms of seasonal variations in 2009, clavicle fractures, distal humerus fractures, both forearm bone fractures, and distal radius fractures showed the highest incidence in summer, followed in order by autumn, spring and winter. Femoral shaft fractures and tibial shaft fractures showed a peak incidence in winter. Distal humerus fractures showed the highest seasonal variation with the highest and lowest incidence in summer (44.5) and winter (24.9), respectively, whereas femoral shaft fractures showed the lowest seasonal variations with the highest and lowest incidence in winter (2.8) and spring and autumn (2.3), respectively (Fig. 3).
Seasonal variation of each fracture was significant. However, in the subgroup analysis, none of the age subgroups showed significant seasonal variation in femoral shaft fracture. Clavicle and distal radius fractures showed significant seasonal variation for all age subgroups (Table 1).
DISCUSSION
Tibial shaft fractures showed a slightly decreasing annual incidence, whereas femoral shaft fractures showed an increasing incidence during the recent five years between 2005 and 2009. Clavicle fractures, distal humerus fractures, both forearm bone fractures and distal radius fractures did not demonstrate any notable increasing or decreasing tendency. Distal humerus fractures showed the greatest age and seasonal variations, and femoral shaft fractures showed the smallest age and seasonal variations. After stratifying the fracture incidence according to age group, distal radius fractures in the 5-9 year age group showed the highest seasonal variation, and tibial shaft fractures in the 0-4 year age group showed the lowest seasonal variation in 2009.
Before discussing the study results, some limitations need to be addressed. First, the age groups were based on administrative factors rather than clinical considerations. If the age groups had been made on a clinical basis, the study results could have had more useful implications in terms of the treatment choice (conservative or surgical) and prognosis. Second, the data of this study was retrieved on a diagnosis basis and not on a subject basis. Therefore, concurrent injuries or other causative factors could not be evaluated. Subject based data is expected to provide more valuable clinical information in a future study.
The variation in the fracture incidence according to age groups is an important issue. This has clinical significance in that the fracture incidence can be affected by developmental factors. The considerable variations in fracture incidence in this study, particularly for distal humerus fractures and distal radius fractures, suggest that the development of anatomical structures or certain types of activity and behavior can be causative factors in terms of the fracture mechanism, fracture sites and fracture pattern.
Many studies have examined the seasonal variation of specific fractures.1-4,6,19) Previous studies have suggested different causes for the seasonal variations in fracture incidence, and these include change in outdoor activity due to weather, change in vitamin D metabolism due to a change in the length of daytime, increase in the slippery load in winter, visual acuity changes in winter due to early sunset, etc.5,9,11,20-28) For the six pediatric and adolescent orthopaedic fractures examined in this study, the highest incidence was observed in summer except for femoral shaft fractures and tibial shaft fractures. Femoral shaft and tibial shaft fractures showed the highest incidence in winter but lower seasonal variation. Therefore, the higher incidence of the four upper extremity fractures in children and adolescents in summer can probably be explained by children and adolescents engaging in outdoor sports activity more often, and sustaining low-energy traumatic injuries that cause the fractures. On the other hand, the higher incidence of the two lower extremity fractures in winter can partly be explained by seasonal factors, such as the higher slippery load, decreased visual acuity and decreased vitamin D metabolism in winter. A considerable portion of femoral shaft fractures and tibial shaft fractures are believed to be caused by high-energy trauma, such as traffic accidents, which are less affected by seasonal factors, but this issue requires further investigation.
A previous study reported a comprehensive survey of the fracture incidence of children in the 0 to 15 years age group.29) Although the age of the study population was slightly different from that of the present study, the incidence of both forearm bone fractures, distal radius fractures and femoral shaft fractures shown in that study was comparable to that obtained in the present study. On the other hand, the incidence of clavicle fractures, distal humerus fractures, and tibial shaft fractures in the present study was much higher than that of the previous study, showing a 2.7 to 3.9 fold increase in incidence. It is believed that ethnic or cultural factors can also play a role in fracture incidence, which is a factor researchers and clinicians should consider.
In conclusion, the four upper extremity fractures tended to show greater variations than the two lower extremity fractures in children and adolescents in a nationwide database of South Korea. The study results are believed to be helpful in the planning and assigning of medical resources for fracture management in children and adolescents.



 XML Download
XML Download