

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Accessory bones are common skeletal variations of the ankle and foot, derive commonly from unfused accessory ossification centers, and may appear to be normal subdivisions of ordinary bones or nearby additional free elements.1) The most common accessory bones of the ankle and foot are the os trigonum, the accessory navicular, and the os intermetatarseum. Other less frequent accessory bones include the os sustentaculi, os supranaviculare, os vesalianum, os calcaneus secundarius, os subtibiale and the os subfibulare.2)
Herein, the author describes a previously unreported accessory bone of foot, which was not encountered even in large series on accessory bones of the feet.1,3) The accessory bone concerned was located between the navicular, medial cuneiform, and intermediate cuneiform, and articulated with the medial cuneiform and the intermediate cuneiform. Accordingly, it was named os infranaviculare.
CASE REPORT
A healthy 45-year-old man was referred to our clinic with an atraumatic 3-year history of pain on the dorsomedial surface of the right foot, which worsened with activity. The pain began as a diffuse dull pain during running, and progressed to an exquisite pain during standing or after a 10-minute walk since 6 months before our clinic visit.
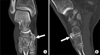
Tenderness was noted around the symptomatic medial midtarsal area. However, no other specific finding was found during a physical examination. His laboratory data, including his uric acid level, were also within the normal range. Radiographs of the right foot revealed a 10 × 15 mm sized accessory bone between the navicular and the medial cuneiform (Fig. 1), but no equivalent in the left foot. Computed tomography (CT) demonstrated that the accessory bone contacted the intermediate cuneiform and the navicular and medial cuneiform; sclerotic change and a bony spur were observed between the accessory bone and the navicular (Fig. 2).
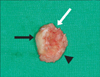
His symptom had not improved despite the 6 months of conservative treatment for pain control, and finally, the accessory bone was excised. Intraoperatively, the tibialis anterior was not attached to the accessory bone, which articulated with the medial cuneiform and the intermediate cuneiform. However, it was connected to the navicular by synfibrosis (Fig. 3). At his 12-month follow-up, the patient reported pain relief during walking, but slight tenderness persisted on the surgical scar.
DISCUSSION
When a patient without a recent trauma history complains of medial side midfoot pain, several types of disease, such as, accessory bones around the navicular, osteonecrosis, and stress fracture of the navicular, and gout may be considered.1,3-6)
The most common accessory bone around the navicular is located on the medial side of the navicular. However, other accessory bones have been sporadically reported around the navicular. An accessory bone between the navicular, medial cuneiform, and intermediate cuneiform is extremely rare. The condition was initially reported by Dwight based on two macerated specimens in 1902, and was named os intercuneiforme.7) The accessory bones were described as rounded, without an articulated connection with surrounding structures, and as being embedded in connective tissue. The incidence rate of os intercuneiforme was reported to be one per 3,754 feet (0.026%) in one series,7) and as one per 3,460 feet (0.029%) in another.3)
In the present case, although the accessory bone was located between the navicular, medial cuneiform, and intermediate cuneiform, it differed from os intercuneiforme, because it articulated with the medial cuneiform and the intermediate cuneiform. The navicular was the only surrounding bone without articulation contacted by connective tissue, which means that the accessory bone was a secondary ossification center of the navicular, and thus, we name it os infranaviculare.
Accessory bones usually remain asymptomatic, but can become painful due to fracture, degenerative change, and avascular necrosis and due to irritation or impingement of adjacent soft tissues.8) In the described case, advanced degenerative change between the navicular and accessory bone was considered to be the main cause of foot pain.
Symptoms caused by accessory bones are initially treated nonoperatively, and thus, we adopted conservative treatment (rest, anti-inflammatory agents, and a shoe insert) for 6 months, but those efforts were futile. Finally, because the patient wanted to participate in sports activities, we decided on surgical treatment. Simple excision is recommended for an accessory bone of the foot and ankle, as long as excision does not create a large defect at the tendon insertion.8) In this case, we were able to simply excise the accessory bone without additional procedures, because the tibialis anterior tendon was not involved.

 XML Download
XML Download