

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Various systems of computer-assisted orthopaedic surgery (CAOS) in total hip arthroplasty (THA) have been developed since the early 1990s. These include computer assisted preoperative planning, robotic devices, navigation, and patient specific surgical templates. The author reviews the scientific literature on these CAOS systems in THA and describes the history, effectiveness and safety issues to help readers to evaluate and compare the pros and cons of these CAOS applications.
SURGICAL ROBOT
The first clinically applied system of CAOS in THA was a robotic system called ROBODOC1) (ISS, Sacramento, CA, USA) (Fig. 1). The concept was developed in the late 1980s because it was recognized that even well designed custom made hips could fail if the implant cavity was prepared inappropriately. The idea was to bring computer-aided design and computer-aided manufacturing (CAD/CAM) into the operating room (OR) for an accurate placement of femoral prostheses. It was conceived as a system with which to assist surgeons to preoperatively select the size and type of cementless femoral implant best suited to the individual patient, to machine the cavity in the bone to tight tolerances comparable to the implant's tolerances for the placement of a press-fit cementless implant in the bone. The ROBODOC system was the first active system, which performs some surgical actions that are programmed preoperatively. It consists of a preoperative planning computer workstation (called ORTHODOC) and the ROBODOC surgical assistant, which has a five-axis robotic arm with a high-speed milling device (end effector) connected to the tip of the arm via a force torque sensor2) (Fig. 1). ORTHODOC 3-dimensional (3D) preoperative planning is performed based on computed tomography (CT) image data that allows surgeons to select the optimal design and size of the femoral component for each patient by comparing the fit and fill of different implants.3) Data, including the optimized plan, are transferred to ROBODOC, which mills the bone cavity to the same dimension as the corresponding rasp after the calibration of the milling bar, rigid fixation of the bone to the ROBODOC, and registration of the femur.
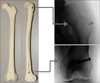
Calibration is a procedure that matches geometric computer models of implants or tools to the coordinates of the positions of the actual implants or tools. Registration is a computational procedure that matches preoperative images or planning information to the position of the patient on the OR table. There are three registration methods.4,5) One is paired point matching registration with which the surgeon must identify three or more points on the preoperative images and the corresponding points on the patient during surgery accurately. This method is not reproducible if anatomical landmarks are used for the matching points. To resolve this irreproducibility, fiducials are placed in the target bones before volumetric (CT, magnetic resonance imaging [MRI], etc.) images are obtained (fiducial-based registration) (Fig. 2). These fiducials are used to create a 3D reference for the patient's bone. The intraoperative locations of the fiducials are used to relate the position of the patient's bone to the preoperative plan. This method is accurate, but requires an additional operation to place the markers. ROBODOC initially used three titanium screw fiducials for registration. These three screws were inserted at the greater trochanter, the medial femoral condyle, and the lateral femoral condyle before taking CT images. In 1998, the number of fiducials was reduced to two by using a pin extension, which provided two points along the condyle screw. Although fiducial-based registration is accurate,2,6) an additional preceding minor operation before THA and fiducial site knee pain are the drawbacks.7)
Shape-based (surface) registration is an alternative method that does not require fiducials. With this method, the point on the computer model, nearest the measured surface point, is designated as the corresponding point, and the calculation is repeated to reduce the average distance between each measured point and the corresponding surface point (Fig. 3). Mathematical calculations are performed using the iterative closest-point algorithm and the least-squares method. To avoid local minima, the baseline registration is performed, using a paired point method to obtain the starting position for registration. A certain number of surface points are then used for the final matching, for which the calculation is repeated until it becomes saturated. Using this surface-matching technique, the shapes of the bone surface model generated from preoperative images are matched to the surface data points collected during surgery. ROBODOC introduced a surface registration method in 1999 and the clinical accuracy of this registration method has been reported to be as accurate as that of the fiducial-based registration method.8) The third method of registration is 2D-3D or 3D-3D registration using intraoperative fluoroscopic images.5,9) Although a 2D-3D registration method was shown to be accurate for robotic-assisted THA in a laboratory setting,5) robotic applications of this registration method have not yet been used clinically.
Several clinical studies using ROBODC in THA have been published. The first one was a Food and Drug Administration (FDA)-authorized multicenter randomized control study conducted in 136 hip replacements in the United States during 1994-1995 after a small feasibility study during 1993-1994. There were no significant differences in the Harris hip scores or short form health survey data between the ROBODOC group and the control group. However, radiographs showed that the fit and positioning of the femoral component were significantly better in the ROBODOC group. The only complication for which there was a significant difference between the groups was intraoperative femoral fracture: three in the control group and none in the ROBODOC group.2) In a German study of 900 hip replacements performed using ROBODOC (858 unilateral hip replacements and 42 bilateral hip replacements, including 30 revision cases) from 1994, there were no intraoperative femoral fractures. In revision THA for cemented stems, the revision software allowed gentle removal of even large, deep cement mantles. Cement removal was safer and faster when performed by the robot than when performed by hand.2,10) Osteonecrosis, due to heat generation from milling of bones, has been mentioned as a possible disadvantage of milling devices (even if irrigation is used with ROBODOC),11) but no adverse clinical effects due to heat generation have been reported. A study of the ROBODOC two-pin registration method for primary THA through a posterior approach showed better clinical scores at two years and better stem alignment on radiographic evaluation in the ROBODOC group than in the manual control group.12) Hand rasping had the potential to cause intraoperative femoral fractures, undersizing of the stem, unexpectedly higher vertical seating, and unexpected femoral anteversion, causing inferior implant fit. In a transesophageal cardioechogram study, robotic milling of the femur showed fewer incidences of pulmonary embolic events than manual rasping.13) A dual energy X-ray absorptiometry (DEXA) study suggested that robotic milling was effective in facilitating proximal load transfer around the femoral component and minimizing bone loss after cementless THA.14) ROBODOC procedures also showed less variance in limb length inequality.15) There was another active robotic system called CASPAR (URS, Rastatt, Germany) that was similar to ROBODOC. However, there are only a few reports of the laboratory testing of CASPAR.16,17) On the other hand, there are some reports on complications of ROBODOC THA procedures. A German study showed problems with an active robotic system of higher dislocation and revision rates than with conventional methods, although hip scores, prosthesis alignment and limb length were better for the ROBODOC group at 6 and 12 months.18) The problems encountered in this study seem to be due to human errors, such as improper selection and positioning of implants, and inappropriate soft tissue protection during an anterolateral approach.19) When the insertion of the hip abductor muscles was protected appropriately, a gait analysis showed no functional impairment after ROBODOC procedures, even through an anterolateral approach.20) There were other reports of technical complications, such as a procedure stop due to bone motion during cutting requiring re-registration, femoral shaft fissures requiring wire cerclage, acetabular rim damage during milling, milling of a defect of the greater trochanter, and registration failures.21,22) These errors and complications encountered with the use of active systems, such as ROBODOC, suggest that no current active system can be considered autonomous, with the implied ability on the part of the robot or system to make decisions. What surgeons do with an active system is to proceed, to pause, or to abort a preoperatively programmed milling procedure being carried out by the robot, while surgeons carefully watch the moving path of the cutter and listen to the sound of the milling. The surgeons need to understand the workspace and appropriate positioning of the robot. Therefore, surgeon training is an important issue that can minimize negative incidences due to the learning curve. For ease of surgeon acceptance, a few semi-active/haptic systems were developed. Acrobot (Acrobot Co., London, UK) is one of them. The drill bit at the tip of the robotic arm is moved by a surgeon's hand, but it does not move outside of the milling path boundary, which is defined according to a 3D-image-based preoperative planning. There is only one report for resurfacing hip.23) RIO (Mako Surgical Corp., Fort Lauderdale, FL, USA) is another semi-active boundary constrained robotic milling system, and recently, it was successfully used to achieve precise acetabular reaming and cup placement.24) Although it is easier for surgeons to accept a semi-active system than an active system, there is still little evidence in the literature about the feasibility, safety, and efficacy of the semi-active systems.
SURGICAL NAVIGATION
Thanks to advances in 3D sensor technology, various types of navigation for THA were developed in the late 1990s. Navigation is a passive system, which does not perform any actions on patients, but only provides information and guidance to the surgeon who still uses conventional tools to perform the surgery. Navigation uses optical sensors or magnetic sensors as 3D position sensors to track the target bones and surgical tools or implants. Optical systems use charged coupled device (CCD) cameras to obtain positional information (Fig. 4), which is usually based on an infrared light from a dynamic reference frame (DRF) with infrared light-emitting diodes (LED) or infrared light reflecting markers. The DRF is attached to the target bones and surgical tools to be tracked. Measurements by optical sensors are highly accurate and fast; and many LEDs can be tracked simultaneously, although an uninterrupted line of sight must be maintained between the CCD camera and DRFs. On the other hand, there is no line of sight problem with magnetic sensors, although there are concerns about their accuracy, which may be reduced by the motor of the OR table or metallic tools. There are three types of navigation in THA: CT-based navigation, fluoroscopic navigation, and imageless navigation.
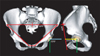
CT-based navigation was first introduced for accurate cup placement in THA by DiGioia et al.25) Preoperative CT images were used for planning. For measurements of cup alignment, pelvic coordinates should be located on the 3D reconstructed CT images, based on the anatomic landmarks, such as the anterior superior iliac spines (ASIS) and the pubic tubercles. A plane through these landmarks called anterior pelvic plane (APP) is often used for pelvic coordinates (Fig. 5). However, because the individual sagittal angle of APP is not always flat in a neutral (zero) position of the hip and it can be affected by an individual's shape, aging, or spinal deformity due to osteoporosis,26) others use a functional pelvic plane where the pelvis in supine on the CT scan table is axially rotated until the bilateral ASISs touches the same horizontal plane, and the interteardrop line is then used as the mediolateral axis (Fig. 5).27,28)
Clinical studies have demonstrated that CT-based navigation provides more accurate measurements of cup alignment than the conventional mechanical instruments; thus, helping to eliminate the malpositioning of cups.26,29) Minimally or less invasive approaches through a small skin incision are a risk factor for cup malalignment, but the accuracy of cup placement with CT-based navigation is not affected by these approaches.30,31) When both pelvis and femur are navigated, limb length, femoral offset and range of motion can be measured intraoperatively.27,28,32) A long term follow-up study showed that CT-based navigation reduces the rates of dislocation and impingement-related mechanical complications leading to revision in cementless THA using ceramic-on-ceramic bearing couples.33)
CT-based navigation is the most accurate,34) but it takes time for preoperative planning on CT images, which increases cost and radiation exposure. This can be one of the barriers for surgeon acceptance. Imageless navigation does not use CT images to guide cup orientation. Instead, after a DRF is attached to the pelvis, pelvic coordinates are created intraoperatively by pointing at landmarks, such as the ASIS and the pubic tubercles to define APP. Several clinical studies demonstrated better cup alignment with the use of imageless navigation than the conventional mechanical instruments.35-40) However, accuracy depends on the technique of landmark pointing and soft tissue thickness on the landmarks.41-44) Moreover, the individual's sagittal tilt is not taken into account when APP is used for the pelvic coordinates.43) Fluoroscopic navigation uses the same concept as imageless navigation in using the landmarks, the positions of which are registered with the fluoroscopic images. However, this registration process is cumbersome and does not show any advantages over imageless navigation.45) There are some papers on imageless navigation for femoral stems and resurfacing hip components.46-50) However, the accuracy of imageless navigation for resurfacing could be affected by femoral deformity, and it may not be accurate enough for hip resurfacing in some cases.51,52)
PATIENT SPECIFIC TEMPLATE AND OTHER INSTRUMENTS
Although robotics and navigation help to improve the accuracy of surgery in THA, broad clinical applications of these systems is hindered by high cost, additional time during intervention, problems of intraoperative man-machine interactions, and the spatially constrained arrangements of additional equipment within the operating room. Patient specific template (PST) is an alternative CAOS method for 3D image-based preoperative planning and precise surgery on bone structures.53) PST has a base part that fits on the bone surface intraoperatively, and a guide part to achieve preoperatively planned alignment of the instruments or implants (Fig. 6). PST has been applied to cup placement guides in THA and femoral guide wire insertion for hip resurfacing.54-58) PST does not require an expensive hardware installation on the part of the hospital. However, it requires preoperative CT images, skill to carry out optimal preoperative planning on CT images, and the expense of producing the template. Moreover, an exact fit of PST to the target bone area is not easily verifiable intraoperatively and it may need a wider exposure through a larger skin incision for PST fitting than navigation surgery. Hip Sextant (Surgical Planning Associates Inc., Medford, MA, USA) is another instrument designed as a guide for acetabular cup orientation during THA.59) This does not require an individual template instead the positions of three-point contact are adjusted, according to the software of CT-based preoperative planning. PST and computer assisted mechanical instruments are still in an early stage of clinical trials and more clinical studies are necessary to evaluate the effectiveness and safety of these devices.
RECOMMENDATIONS
Finally, it is important to understand the pros and cons of each CAOS system and readers should know that CAOS is a useful tool to help surgeons perform accurately what surgeons want to do in order to better achieve their clinical objectives. Thus, it is important that the surgeon fully understands what he or she should be trying to achieve in THA for each patient. The outcomes of THA depend on both the objective of the surgery and the accuracy of the surgery.




 XML Download
XML Download