

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Open reduction and volar plate fixation for distal radius fractures is becoming very popular, but several reports have documented complications associated with volar plating.1) Extensor tendon rupture after volar plating is a relatively common complication,2,3) but flexor tendon ruptures have rarely been reported. Most reported instances of a flexor tendon rupture have involved improper plate placement, increased prominence of the distal edge of the plate because of collapse of the fracture site, use of custom-made plates, current steroid use by the patient, or a history of tendon injury.4-9) We report a case of delayed rupture of the flexor pollicis longus (FPL) tendon 40 months after volar plating with a 3.5-mm T-locking compression plate (T-LCP, Synthes, Paoli, PA, USA).
CASE REPORT
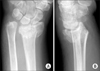
A 63-year-old right-handed woman sustained a right intra-articular comminuted distal radius fracture with dorsal displacement (Fig. 1), a right femoral shaft fracture, and a hemothorax in a motor vehicle accident. Open reduction and internal fixation was performed using 3.5-mm T-LCP for the distal radius fracture at 12 days after the trauma, and the plate was covered by the pronator quadratus after fixation. Immediate postoperative plain radiographs revealed acceptable restoration of radial inclination, radial length, and volar tilting, except an approximate 2 mm step-off of the articular surface. The plate was placed tightly to the distal radius without any gap, and even though the distal edge of the plate was very close to the transverse ridge of the distal radius, it did not reach the distal portion of the transverse ridge. Plain radiographs at 8 months after surgery revealed bony union without further collapse of the distal fragment compared to that of the immediate postoperative radiographs, and range of motion of the right wrist was normal. Accordingly, we recommended plate removal, but the patient refused, stating that she was experiencing no specific discomfort.
She visited our hospital at 40 months after surgery and reported that she had a sudden thumb flexion limitation during washing 10 days ago. She had no associated pain and no warning symptoms such as tendon irritation. A physical examination revealed that she could not actively flex the right interphalangeal joint of her thumb, although the range of motion of her other joints and sensory findings were normal. Radiographic findings revealed no definite interval change (Fig. 2). Ultrasonographic findings showed that the FPL tendon had ruptured, and the proximal stump was found at the radiocarpal joint. We performed a surgical exploration and found that the distal edge of the plate was exposed even though the pronator quadratus was nearly completely covering the plate. The FPL tendon had ruptured over the distal edge and was frayed (Fig. 3). We performed complete debridement of the granulated and frayed tissue in the ruptured margin, removed the plate, and performed a primary repair of the tendon using the modified Kessler method. The patient wore a thumb spica cast for 3 weeks and then began passive-motion exercises. The patient had no movement restriction of the right thumb at 6 months after surgery.
DISCUSSION
When a plate is fixed on the dorsal side, it causes various complications such as extensor tendon irritation or rupture and metal breakage due to the difficulty of manufacturing a plate to fit the irregular bone contour.2,3) In contrast, volar plating significantly reduces these complications, but reports have been published on the complications associated with volar plating, including complex regional pain syndrome, carpal tunnel syndrome, tendon injury, or infection.1,6,7) Most reports of complications related to volar plating have considered extensor tendon damage; in particular, damage to the extensor pollicis longus. Flexor tendon injuries after volar plating are extremely rare.
Orbay and Touhami10) emphasized the importance of the transverse ridge or watershed line of the distal radius to prevent a flexor tendon injury. Plates placed distal to the transverse ridge have the potential to impinge on the traversing flexor tendons. Bell et al.4) reported their experience with four patients who had FPL ruptures after volar plating and noted that all patients were taking steroids. They concluded that steroid use is an indication for early removal of the device. Additionally, they recommended that volar plates be removed early if they are placed on the distal part of the distal radius transverse ridge or if the distal edge of the plate becomes prominent because of collapse of the fracture site, as these conditions could result in irritation to the tendon. Cross and Schmidt5) reported their experience with two patients who had FPL ruptures after their fractures were repaired by volar plates manufactured by two different companies. They also emphasized the role of placing the plate in relation to the transverse ridge for a tendon rupture due to friction. They recommended that volar plates be removed early and that patients be advised of the possibility of FPL damage if simple radiographs revealed that the plates were located on the distal part of the transverse ridge. Duncan and Weiland6) reported their experience with a patient whose FPL ruptured 9 months after surgery and noted that the distal part of plate adhered tightly to the bone without a gap. They emphasized that the plate edge must be covered with the pronator quadratus to prevent irritation to the tendon (Table 1).
In our case, there was no long-term use of steroids and the Synthes 3.5-mm T-LCP used was widely available and not custom-made. Additionally, no history of injury before surgery or of thumb abnormality after surgery were noted. Follow-up plain radiographs revealed bony union without further collapse of the distal fragment, as compared with radiographs obtained immediately after surgery. However, even though the plate was not violating the distal part of the transverse ridge, it was at the transverse ridge level. We found that the plate shaft was covered by the pronator quadratus, but that the distal edge was exposed. Additionally, the FPL tendon ruptured right at the point where it met the exposed distal edge. We suggest that the rupture was due to friction from the exposed distal edge of the plate at the transverse ridge, because the pronator quadratus does not attach to the distal part of the transverse ridge. Therefore, we believe that it is very important for the distal edge of a plate to be completely covered by the pronator quadratus to prevent a flexor tendon injury.
As reported by some authors, when the FPL ruptures because of friction against the plate over a long period of time, primary repair is impossible in most cases because of a hypertrophied tenosynovium and a tendon defect with fibrous tissue and retraction; thus, a tendon graft or tendon transfer is necessary. However, although the rupture in our patient occurred 40 months after the initial surgery, findings from the exploratory surgery revealed little retraction; thus, a primary end-to-end repair was possible even after removing some fibrous tissues and a frayed tendon. It is unclear why such unusual circumstances occurred.
We have found that when the plate is located near the transverse ridge after surgery, it is necessary to make thorough and careful observations to prevent flexor tendon damage. If symptoms such as tendon irritation occur in this situation, surgeons should consider removing the plate as soon as possible after bony union is achieved.



 XML Download
XML Download