

 PDF
PDF ePub
ePub Citation
Citation Print
Print


High flexion of the knee after total knee arthroplasty is essential for a successful overall functional outcome.1-3) One problem of total knee arthroplasty in Asian people is that patients cannot flex the knee beyond 120° following the operation. Various factors that may influence the range of motion of the knee after a total knee arthroplasty have been postulated. There have been increasing complaints especially from Asian patients regarding the difficulties associated with carrying out their daily activities, whose life style involves sitting on the floor with their legs crossed or in the kneeling position.1,4) The high flexion posterior stabilized mobile bearing knee prosthesis has been introduced to enhance knee flexion. We evaluated the results of total knee arthroplasty using high flexion rotating platform mobile bearing knee system in Korean patients and compared the results of this new prosthesis total knee arthroplasty with those of total knee arthroplasty using standard rotating platform mobile bearing knee system in order to assess the clinical results including the maximal flexion angle after a follow-up of at least 2 years.
METHODS
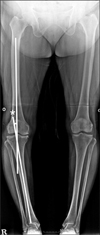
From February 2006 to February 2007, the senior author (YBJ) performed one hundred seventy-two consecutive primary total knee arthroplasties in one hundred twenty-four patients. The bilateral total knee arthroplasties were performed in forty-eight patients (96 knees) who received the Low Contact Stress rotating platform (LCS RP) mobile bearing knee prosthesis (DePuy, Warsaw, IN, USA) total knee component on one side and the Press Fit Condylar Sigma rotating platform high flexion (PFC Sigma RP-F) on the contralateral side (Fig. 1). One hundred ten total knee arthroplasties were performed with LCS total knee component and sixty-two with PFC Sigma RP-F. Of them, total knee arthroplasties with LCS anteroposterior glide total knee components (17 knees) were excluded in this study. Patients were excluded if they had body mass index score over 30 and valgus knee deformity. All patients had minimum of 2-year follow-up. The mean duration of follow-up was 2.9 years (range, 2.0 to 4.3 years). So, one hundred eleven knees were available for inclusion in the study. Institutional Review Board approval for the design and protocol of this retrospective study was received. Sixty-one knees were treated with LCS RP total knee component and fifty knees with PFC Sigma RP-F. Thirty-five patients received bilateral total knee arthroplasties. We compared the demographic data between sixty-one knees of LCS RP group and fifty knees of PFC Sigma RP-F group (Table 1).
There were 60 women and 1 man with a mean age of 68.9 ± 6.0 years (range, 52 to 81 years) in LCS RP group and 45 women and 5 men with a mean age of 68.4 ± 5.9 years (range, 55 to 86 years) in PFC sigma RP-F group. The diagnosis was all osteoarthritis in this study. All surgeries were performed by the same surgeon (YBJ) using a modified subvastus approach through a midline skin incision measuring about 10 cm in length.5) In modified subvastus approach is just 2-3 cm additional snip at tendinous junction of the vastus medialis obliquus. The cruciate ligaments were excised in all patients in both groups. All knees in this study had total knee arthroplasties with use of computer-assisted surgical navigation. Soft tissue balancing was performed using a sequence of tissue releases for medial, lateral and posterior structures.
The postoperative protocol for both groups was identical. We encouraged straight leg raising exercise right after the operation and all patients began weight bearing with crutches or a walker and range of motion exercises on the second day after the operation.
Clinical and radiographic evaluations were done at six weeks, three months, six months, and one year after the operation and then yearly thereafter. Standing AP, lateral, and Merchant radiographs were evaluated according to the system of the Knee Society for radiolucencies at the bonecement interface, wear of polyethylene, any change in the position of the component, alignment, and osteolysis. The Knee Society score and the Hospital for Special Surgery (HSS) score were calculated preoperatively for all patients and at the time of final follow-up for all patients who returned to the clinic. In addition, each patient completed a self-administered questionnaire which included the Short Form-36 (SF-36) health survey. The active range of motion was determined with use of a standard clinical goniometer.
Statistical Analysis
The range of motion and the scores of the clinical results are presented as means with ranges and standard deviation.
Two blinded reviewers (JJH and CHY) independently reviewed range of motion and radiologic parameters of all patients on two separate occasions. There was no communication between the reviewers. We assessed interand intra-observer reliabilities for range of motion and radiologic parameters including tibiofemoral angle (Fig. 2), patellar tilt (Fig. 3), and posterior femoral condylar offset (Fig. 4) using interclass correlation coefficients. Intraclass correlation coefficients were interpreted as follows: < 0.20, slight agreement; 0.21-0.40, fair agreement; 0.41-0.60, moderate agreement; 0.61-0.80, substantial agreement; and > 0.80, almost perfect agreement.
The chi-square test with Fisher exact test was used for categorical variables and the t-test for numerical variables. Null hypotheses of no difference were rejected if two-sided p-values were less than 0.05. Data were analyzed statistically using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Clinical Results
Knee score
The preoperative knee scores did not differ significantly (Table 2). There were no statistically significant differences between groups in the Knee Society Score (KSS), function, and the HSS scores postoperatively. In the LCS RP group, the mean postoperative final follow-up KSS knee score was 93.72 points, KSS functional score 77.29 points, and HSS score was 90.19 points. In the PFC Sigma RP-F group, the mean postoperative final follow-up KSS knee score was 93.54 points, KSS functional score 77.60 points, and HSS score was 89.86 points. The postoperative pain scores, according to both knee-scoring systems, did not differ significantly between the groups (p = 0.446 and p = 0.118, respectively) (Table 3).
Pain
Of the sixty-one knees treated with the LCS prosthesis, forty-five (73.7%) were not painful and sixteen (26.2%) were mildly painful (no effect on daily activity) at the time of the latest follow-up. Of the fifty knees treated with the Sigma RP-F prosthesis, thirty-six (72%) were not painful, fourteen (28%) were mildly or moderately painful, and none were severely painful at the time of the latest follow-up examination. There was no significant difference between the two groups (p = 0.834).
Range of motion
Preoperatively, the mean knee flexion contracture was 6.7° (range, 0° to 25°) in the LCS group and 9.3° (range, 0° to 40°) in the Sigma RP-F group. No knee in either group had a range of motion of < 75° preoperatively or postoperatively. Sixty knees (9.8%) in the LPS group and five knees (10%) in the Sigma RP-F group had a range of motion of < 110° at the time of final follow-up. Maximum flexion in both groups was 150° in the LPS group and 145° in the Sigma RP-F group. At the time of final follow-up, the range of knee motion did not differ significantly in either group (p = 0.637) (Table 4).
Radiographic Results
There were no significant differences between the groups with regard to radiographic parameters, except in the preoperative, final follow-up femorotibial, and final follow-up posterior condylar offset (Table 5). No knee had aseptic loosening of the femoral, tibial, or patellar component, and no knee had subluxation or dislocation of the tibiofemoral joint or a patellar dislocation.
DISCUSSION
Mobile bearing total knee arthroplasty designs offer the theoretical advantage of increased implant conformity and contact area while minimizing stresses transmitted to the fixation interface.6) The dual articulation is also designed to reduce polyethylene wear and to subsequently decrease the rate of revision total knee arthroplasty. This uncoupled motion through the tibial tray polyethylene bearing articulation theoretically minimizes the transfer of torsional stresses to the fixation interface that is present with fixed bearing total knee arthroplasty prosthetic designs. Many studies have been conducted on comparison of the fixed-bearing and mobile bearing total knee arthroplasty.7-10) However, there is a paucity of information in the literature regarding comparison of rotating platform and high flexion rotating platform total knee arthroplasty. So, we compared the results of PFC Sigma RP-F total knee arthroplasty with those of total knee arthroplasty using LCS mobile bearing knee system in order to assess the clinical results including the maximal flexion angle after a follow-up of at least 2 years.
The range of motion after total knee arthroplasty rarely exceeded 120°.2,11,12) In a prospective, observational multicenter study of 684 patients, Miner et al.13) reported that there was no significant difference in satisfaction and perceived quality of life in patients who obtained greater than 95 of flexion after total knee arthroplasty than those who exhibited less than 95 of flexion at 12 months' follow-up. Meneghini et al.14) reported that there is no statistically significant benefit in overall knee function in terms of the mean Knee Society and function scores for those patients who attained high flexion greater than 125 and those who attained normal flexion after total knee arthroplasty. However, in the Asian life style, hyperflexion of the knee is necessary for daily living. In order to sit on the floor with crossed legs, the flexion of the knee joint should be more than 120° and more than 135° of flexion are required to sit down in kneeling position. To enhance knee flexion, several new designs were introduced. Among them, the new PFC Sigma RP-F knee is designed to provide range of motion of 155° without increasing contact stresses in the polyethylene by providing a third articulating surface and simultaneously allowing for proper patellar tracking. In the current series, mean postoperative range of flexion at last follow-up did not differ significantly between the two groups. The final follow-up mean maximum flexion angle was 125.6 in the LCS RP group and 127.0 in the PFC Sigma RP-F group (p = 0.620).
Several factors may have played an important role in the achievement of this high degree of flexion, including the preponderance of women, the low body mass index of the patients, the use of the subvastus approach, the relatively good preoperative range of motion, and the effective restoration of the joint line.15,16) Li et al.12) showed that the cam-spine interaction may affect posterior femoral translation only at flexion angles between 90° and 135°. Beyond this range of flexion, cam-spine engagement was not observed consistently. Despite the absence of engagement additional posterior femoral translation was found to occur as the knee flexed to higher angles. They speculated that compression of the posterior soft-tissue structures (such as the posterior capsule, pericapsular fat, muscle, and skin) may act to push the tibia anteriorly resulting in continual posterior femoral rotation of the total knee replacement at higher flexion angles. So the posterior femoral translation may not be sufficient to achieve higher knee flexion in patients. Additional factors are likely to play an important role in permitting the reconstructed knee to achieve higher flexion.
Design concepts for high flexion in the new PFC Sigma RP-F knee are focusing on shortening radii of curvature, thickening of posterior femoral condyle, increasing of the height of the posterior-stabilized box and deepening the trochlea groove. More bone loss of femoral condyle in the new PFC Sigma RP-F knee is required for these design trends than in the LCS knee. These design changes result in a significant bone loss at revision surgery, excessive polyethylene wear, patellofemoral joint problem and knee instability.17) Once the posterior cruciate ligament is cut, options to prevent anteroposterior instability area limited to the use of a posterior stabilized design with a tibial post and femoral cam, or a dished polyethylene insert with a raised anterior lip.18) In a computational kinematic study, Morra et al.19) reported that in general, all of the designs that did not employ a tibial post and femoral cam mechanism developed tibiofemoral contact in the central or anterior portion of the tibial insert, thus decreasing the capacity to achieve deeper flexion. The incorporation of a central polyethylene tibial post and a horizontal femoral cam serve as a mechanical substitute for the posterior cruciate ligament, to induce femoral roll-back in knee flexion. However, some retrieval studies of posterior-stabilized knee arthroplasties obtained at the time of revision surgery have shown the occurrence of tibial post wear. Puloski et al.18) reported in qualitative and quantitative wear analysis that posterior stabilized implants may contribute to the production of additional wear debris and hence may influence the prevalence of negative outcomes such as osteolysis, aseptic loosening, and reactive synovitis. Mikulak et al.20) found that the vector sum of the tibiofemoral forces and the cam post forces is compression into the tibia. And rotational stresses can be transmitted to the modular interfaces and to the metal cement interfaces. Some described the cases of tibial post fracture.21-23) The failure mechanism of post fracture in that study was presumed to be caused by repetitive anterior impingement between the metal femoral cam and the polyethylene post.
This study had some limitations. First, this study is retrospective. Second, the number of patients is relatively small and the duration of follow-up is short. So we can draw no conclusions regarding the theoretical advantage of the Sigma RP-F prosthesis regarding wear. Despite of these limitations, we concluded there is no need for using high flexion knee design that need more bone removal if there is no advantage in clinical results.







 XML Download
XML Download