

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Among several surgical factors associated with cuff healing, secure tendon fixation to bone is a critical process for successful structural outcome.1) In an effort to improve the biomechanics of rotator cuff repair constructs, tranosseous-equivalent (suture bridge) technique has been proposed and recently become a popular method for rotator cuff repair. In addition, suture bridge repair procedures continue to evolve as instruments and related techniques improve. A variety of anchors has been developed for medial and lateral row fixation. For medial row fixation, in particular, modified suture techniques have been mainly introduced.2) When using a standard method of the suture bridge technique, the medial row suture is generally tied in a horizontal mattress configuration. However, when tendon quality is poor, a horizontal mattress stitch may not be strong enough to hold the rotator cuff tendon tissue. In addition, there may be the possibility of strangulation and relatively quick necrosis of the rotator cuff tendon at the medial row. Historically, many stitch methods were proposed for improving tissue holding in tendon repair.3,4) Among them, the modified Mason-Allen stitch has been recognized as a stronger tissue-holding stitch with less strangulation than other techniques.4) Therefore, we designed a new method of suture bridge technique for medial row fixation using a modified Mason-Allen stitch instead of a horizontal mattress stitch to improve tissue holding and to reduce a risk of strangulation of the rotator cuff tendon at the medial row.
TECHNIQUE
Four portals were typically required for Mason-Allen suture bridge repair: posterior and posterolateral portals (viewing portals) were used mainly for the standard 30 degree angled 4-mm arthroscope, while anterosuperior and lateral portals (working portals) were used for the instruments. After finishing subacromial decompression, release of the cuff, and tissue preparation, the posterolateral portal was used as a viewing portal for the 'Grand Canyon' view. The posterior and anterosuperior portal were used as 'waiting room' portal. After fixating a anchor at the medial row, a Banana SutureLasso (Arthrex, Naples, FL, USA), which was introduced through 'three-sister portals'5) at 45° to the skin and directed toward the midpoint of the lateral border of the acromion, will enter the subacromial space parallel to the rotator cuff as well as perpendicular to the torn edge.
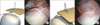
By manipulating the direction of the handle, the edge of the rotator cuff tendon can be pierced with ease. The cuff is slightly lifted with the tissue grasper to make a vertical path of the SutureLasso through the rotator cuff, avoiding an oblique path to the extent possible. The point through the tendon were as medial as possible, ideally 10 to 12 mm medial to the lateral edge of the rotator cuff tear, to maximize the amount of lateral tendon available for compression. A SutureLasso acts as a suture relay to retrieve one limb of the nonabsorbable suture. A No. 1 polydioxanone suture (Ethicon, Somerville, NJ, USA) was passed through the SutureLasso. First, one limb of the nonabsorbable suture is passed in articular-to-bursal direction by a shuttle relay through the tendon (Fig. 1A). The passed limb of suture is retrieved through the lateral portal. For the 2nd passage, the SutureLasso is passed through the cuff at 1 cm from the 1st passage and the suture limb retrieved through the lateral portal is passed in the bursal-to-articular direction by the same method. Then, a horizontal loop is made in the bursal surface of the cuff (Fig. 1B). The passed limb of suture, situated at the articular side, is retrieved again through lateral portal. For the 3rd passage, a SutureLasso should be passed just medial to horizontal strand situated at the bursal side of the cuff. The shuttle relay is used to pass the limb in the articular-to-bursal direction and form a modified Mason-Allen stitch (Fig. 2A). After then, the non-passed limb of suture is passed near to 3rd passage point of previously passed limb, just medial to horizontal loop. As a result, one limb is passed through the cuff 3 times; the other limb, one time (Fig. 2B). If the number of suture anchors used for the medial row increases together with the number of modified Mason-Allen stitches because of a large tear size, the limbs of stitch are retrieved through a posterior or anterosuperior portal to prevent the stitches from getting tangled. The suture limbs were then used to create suture bridges over the tendon. The anchor placement in the anterior-posterior direction is determined by the size of the rotator cuff tendon tear; the anchors should be placed as far anteriorly and posteriorly as possible, in order to maximize the pressurized contact area. The lateral fixation points are placed 1 cm distal-lateral to the lateral edge of the tuberosity footprint insertion (Fig. 3). One thing to note here is that the simple stitch limb that passed through the cuff only once (red color in figure) has to be pulled enough to make the cuff fixed with the modified Mason-Allen stitch contact the medial portion of the foot print before lateral fixation. The limb that passed through the cuff three times to form the modified Mason-Allen stitch can be semi-locked to the cuff and not tightened further. Thus, the simple stitch has to be pulled to tighten before lateral row fixation. If this step is omitted, medial fixation will become loose and the foot print compression of the cuff may be inadequate. Another thing to note is that the simple stitch limb should be tightened only after all the modified Mason-Allen stitches are completed in the medial row. If the simple stitch limb is tightened immediately after completing one respective modified Mason-Allen stitch, the space under the cuff will narrow, making it difficult to perform the next modified Mason-Allen stitch.
The configuration of the modified Mason-Allen suture bridge is essentially a knot-less technique, consisting of modified Mason-Allen stitch with tissue grasping at the medial row and trans-osseous equivalent fixation at the lateral row. The modified Mason-Allen stitch is made by contiguous loops of one limb and the other limb passed the cuff just medial to the transverse loop of modified Mason-Allen stitch, which acts as a rip-stop.
DISCUSSION
In an effort to prevent retears, arthroscopic instruments and operative techniques have changed with time. One of the changes is the introduction of the concept of footprint reconstruction, which resulted in the use of double-row repair that provided a wider interface between the tendon and the original footprint of the humeral head.6) More recently, a suture bridge repair technique has received great attention.7) Some studies have shown superior biomechanical characteristics with a suture bridge repair when compared with a double-row repair.8) In addition, a suture bridge repair reconstructs the footprint of the rotator cuff better than a double-row repair.8)
In single row repair model, tissue holding is a major concern because most retears occur through cuff tissue of poor quality that has poor suture-holding properties. Based on 22 revisions of open suture anchor rotator cuff repairs, Cummins and Murrell9) described that the predominant mode of failure was the suture pulling through the tendon. When using a standard method of suture bridge technique, the medial row suture is generally tied in a horizontal mattress configuration. The suture limbs are then used to create suture bridges over the tendon. Suture bridge repair relies on medial tendon for fixation. Park et al.7) believed that the medial suture passes take advantage of more healthy tendon for fixation strength, because the lateral tendon tissue is often compromised.
Several efforts have been made to improving tissue holding in suture-bridge technique. Toussaint et al.2) developed the 'modified lasso-loop stitch' in medal row repair. However, they advocate the lasso-stitch to be used for smaller tears because of the risk of premature failure of the weakest link in the tendon-suture interface. The loop stitch has significantly lower failure strength when compared with the modified Mason-Allen stitch, as well as horizontal mattress suture of standard suture bridge technique.4)
Historically, many stitch methods were proposed, such as Kleinert, Kessler, Mac or Bunnel, modified Mason-Allen stitch, etc. for tendon repair.4,10) In a comparative study about the ultimate tensile strength of tendon-grasping techniques by Gerber et al.,4) the simple stitches and the mattress sutures slipped out at moderate loads, but the modified Mason-Allen stitch allowed the least gap formation and showed high ultimate tensile strength.
The Mason-Allen suture bridge technique has several advantages: 1) it has a very strong tissue holding property; 2) it creates a rip stop that prevents tendon pull-out; 3) a possibility of strangulation of the rotator cuff tendon, impingement or irritation that may be caused by the knot is low.
This article introduces a new method of suture bridge technique, which occupies the modified Mason-Allen stitch in medial row fixation. Even though the study of biomechanical properties of Mason-Allen suture bridge technique was not performed, we have commonly used the Mason-Allen suture bridge repair technique for rotator cuff tears and obtained secure fixation in the medial row and good interconnectivity configuration over the footprint. We advocate this technique in medium to large-sized rotator cuff tears with relatively poor tissue quality, to increase tissue holding strength.


 XML Download
XML Download