

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Avulsion fractures of the calcaneal tuberosity are rare and infrequent injuries. Recent studies on the epidemiology of these specific fractures have demonstrated that avulsed calcaneal fractures account for 1.3% to 2.7% of all calcaneal fractures.1,2) Due to the low percentage of incidence, little has been reported regarding these types of fractures.
Avulsion fractures of the calcaneal tuberosity are usually caused by sudden muscular contraction of the Achilles tendon when the heel is flat on the ground. Because the Achilles tendon has the following criteria including 1) a broad based insertion on the calcaneus, 2) a braided and coiled anatomical pattern with 90° rotated collagen fibers, and 3) a variable and sudden distribution of force on each avulsion, the resulting patterns of avulsion fracture are as diverse as the potential patient treatment options.3-5) Due to this variability, a modified classification is required according to each type of fracture pattern. Through this report, we propose a novel modified classification system that corresponds to the magnetic resonance imaging (MRI) and surgical findings. The classification scheme defines the four types of avulsion fracture of the calcaneal tuberosity through features including age, gender, the anatomical variances of the Achilles tendon, the fibers involved, and finally the mechanism of injury.
METHODS
Patient Demographics
Patient information was obtained over a six year period from 2003 and 2009 and included a description of the specific trauma episodes, surgical records, X-rays and MRI of all patients with avulsion fracture of calcaneal tuberosity. Twenty patients with an avulsed calcaneal tuberosity out of a total of 764 cases of calcaneal fractures (2.6%) were identified including fourteen men and six women. All patients had an observable avulsed bony fragment on the heel. Adequate X-rays and clinical notes were available for each patient included in the study. Other data included demographic information, the specific mechanism of injury and the anatomical variance of the Achilles tendon according to the findings of both the MRI and surgery.
The mechanism of injury was recorded and defined as tripping, falling or a direct blow. Anatomical variances of the Achilles tendon were previously described as differences in the level of insertion (more or less extensive) of the Achilles tendon into the calcaneus.6) Therefore, anatomical variances of the Achilles tendon were divided into the infrabursal insertion, which is the usual anatomy and more extensive insertion or higher than what is normally described.
Classification
A previous report by Beavis et al.3) proposed a type I to III classification scheme for avulsion fractures of the calcaneal tuberosity. We modified this specific study through the addition of another avulsion type IV fracture (Fig. 1). The type I fracture is a 'simple extra-articular avulsion' fracture (8/20 cases). Type II is the 'beak' fracture in which there is an oblique fracture line running posterior from just behind Bohler's angle (5/20 cases). Type III is the infrabursal avulsed fracture by superficial fibers from the middle third of the posterior tuberosity. In the type IV fracture there is the 'beak', but a small triangular fragment is separated by deep fibers only from the upper border of the tuberosity (3/20 cases). All of the included calcaneal avulsed fractures were classified using the aforementioned criteria (Figs. 1 and 2).
Statistics
Data were analyzed using the SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). For continuous variables, statistical significance was determined using the Mann-Whitney U-test; categorical variables were examined with the chi-square or Fisher's exact test when cell counts were less than or equal to five. A review of the functional end results was not included in this study.
RESULTS
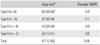
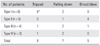
Twenty avulsion fractures of the calcaneal tuberosity were selected and reviewed out of 764 calcaneal fractures (2.6%). The type I fracture was the most frequently observed (40%) and was found more likely to occur in elderly women (Table 1). However, type II, III, and IV fractures were observed more often in relatively younger male patients. This difference in age and gender were significant when comparing type I fracture with the three other types of fractures (p = 0.010, p = 0.018). The fracture patterns were then compared according to the mechanism of injury (Table 2). Type I fractures were more likely to occur by minor trauma such as tripping. However, the occurrence of type II, III, and IV fractures were usually observed in incidents involving more severe trauma (p = 0.019). A direct blow to the bone was the dominant cause of type II fractures and falling for type III and IV fractures.
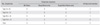
Extensive insertion of the Achilles tendon was found for all types of fractures analyzed (15/20) (Table 3). However, the involvement of fibers of the Achilles tendon varied according to each fracture pattern. All the fibers of the Achilles tendon were involved in type I and II fractures, but only the superficial fibers were involved in type III fractures and the deep fibers in type IV fractures respectively (Fig. 2). These observations imply that the insertion pattern was not related to the fracture type, but rather to the specific fibers that were involved.
DISCUSSION
Several studies have suggested that avulsion fractures of the calcaneal tuberosity have an osteoporotic origin.7,8) These fractures have also been observed with increased frequency in diabetic patients due to insufficiency fractures associated with peripheral neuropathy.9,10) However, this description can only account for the classification of type I fractures within our study and cannot explain the other fracture patterns detected in young male patients. We examined this problem by examining the anatomical variations of the Achilles tendon insertion and the different mechanisms of injury. Although the true prevalence of extensive insertion of the Achilles tendon is not well established, a recent study by Lowy6) demonstrated this anatomical variant in two of ten dissected specimens. In our study, extensive insertion was found in fifteen out of a total of twenty cases of avulsed calcaneal fractures. We hypothesize that individuals that possess extensive insertion are at increased risk for potential avulsion fractures.3) One potential explanation includes the direct force provided by the wide and broad insertion of the Achilles tendon in these individuals and may result in an increased risk of avulsion fractures. However, we found that avulsion fractures could occur through partial involvement of the fibers of the Achilles tendon as according to our surgical and MRI analysis (Fig. 2). Specifically, type III and IV avulsion fractures occurred in patients with extensive insertion but only if the fibers are partially involved with an intact Achilles tendon mechanism. It is interesting that a mechanism to explain partial avulsion fractures was already suggested by Lowy.6) A potential explanation is that a few deep fibers of the tendon, and possibly the fibers arising from the soleus, may tilt the fragment while the rest remain distally attached. When the knee is in a flexed position with the gastrocnemius released, the contraction of the soleus muscle to the heel may induce the type IV type of fracture. We can hypothesize that the mechanism of injury for the type III fracture is similar. The type III fracture is believed to occur when the superficial fibers of the tendon are involved (Figs. 2 and 3).
The mechanism of injury also differs with each classification of fracture described. The type I fracture is more likely to occur as a result of minor trauma such as tripping. However, type III and IV fractures are likely to occur through more severe trauma such as falling down. This indicates that the type I fracture is an insufficiency fracture, however, type III and IV fractures mainly occur due to strong muscular contraction with the heel fixed to the ground. If the strong force of muscular contraction is combined with a direct impact injury, then type II fractures usually occur.
Through the course of our study, we found several limitations that need to be addressed. First, this report is retrospective and therefore contained biases less likely to occur in a prospective study. In addition, our sample number was small due to the low incidence of avulsion fractures of the calcaneal tuberosity. However, most of the literature regarding the avulsed calcaneal fracture involves case reports and explanations of the fracture patterns which are heavily dependent on the opinion of individual authors. Our results demonstrate that the fracture pattern is determined by bone quality, the mechanism of injury and the fibers of the Achilles tendon that transmit the force. We believe that our novel classification system is useful because the treatment options will depend on the specific fracture (Fig. 3). Screw fixation is a good choice for treatment of type I and II fracture because the bony fragment remains of sufficient size for this treatment.4) In type II fractures, however, the posterior skin of the heel must be evaluated quickly, and if it is observed as tented or branched, the fracture must be reduced and fixed. These patients are at risk for skin necrosis of the posterior heel if they are not immediately treated.11) Type III and type IV fractures can be treated conservatively due to the preserved function of the Achilles tendon. However, since these fractures often occur in young individuals, surgical treatment is recommended for maintaining athletic ability. Suture anchor fixation provides superior treatment to screws due to the presence of small bony fragments for type III.5) In two patients included in the study, surgery was completed utilizing suture anchors type IV injuries. The surgery was difficult in the approach to deep fibers and in the management of fragments involved, leading to inferior treatment for the type IV as opposed to type III fractures. Based on our observations, we recommend conservative treatment for type IV fractures.
In summary, we observed four types of avulsed calcaneal fractures and developed criteria for further classification. The fracture patterns are created through osteoporosis, the mechanism of injury and fibers of the Achilles tendon that transmit the force.



 XML Download
XML Download