

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Although femoral head fractures are usually the result of a high velocity injury and occur almost exclusively with hip dislocation, a few cases of femoral head fractures without hip dislocation have been reported.1-3) Here, we present another case of a femoral head fracture that occurred during a fall while playing soccer without evidence of hip dislocation. We also describe atypical features of the fracture using three-dimensional computed tomography (3D-CT) and magnetic resonance imaging (MRI) which were performed at the time of injury and at a nine-month follow-up.
CASE REPORT
A 21-year-old healthy military recruit fell down without external force while playing soccer. His right hip was in flexion, external rotation, and abduction with knee extension during the injury. The patient experienced severe hip pain and was unable to continue playing. He described feeling that his right hip had been displaced from its joint momentarily and that this feeling had subsided spontaneously. Following the injury, he could not bear weight due to pain. When he presented at our emergency room, the neurovascular status of the affected extremity was normal. A physical examination revealed general ligament laxity. His thumb could be passively brought to the palmar aspect of the forearm, and he was able to hyperextend the elbow about 15°. Plain radiographs showed no definite fracture or dislocation but did reveal a cortical defect at the superior aspect of the fovea of the right femoral head (Fig. 1).
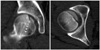
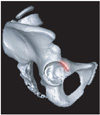
CT revealed a femoral head fracture with a wedge-shaped cortical depression at the superomedial aspect of the femoral head (Fig. 2). 3D-CT reconstruction of the isolated right femoral head roughly indentified the outline and direction of the fracture. The superior cortical cleft was directed from the posteromedial to the anterolateral aspect of the femoral head (Fig. 3). MRI revealed joint effusion, femoral head fracture with bone marrow edema, possible superior capsular avulsion at the anterolateral aspect of the hip joint, and inferior capsular redundancy filled with joint effusion. It also showed a wedge-shaped the femoral head. The indentation appeared to be caused by impaction of the femoral head against the anterior edge of the acetabular rim and to be closely analogous to a Hill-Sachs lesion of the humeral head. The fracture line extended to the inferior portion of the femoral head with bone marrow edema (Figs. 4A and 5A). The patient was admitted and remained in bed for 2 weeks. He was then discharged with a recommendation that he use crutches and not bear weight for three months. A follow-up MRI was performed 7 months after the injury. It revealed that the femoral head fracture was healing with residual reactive bone marrow edema and osteochondral depression. There was no evidence of avascular necrosis of the femoral head. The capsular lesion observed on the post-admission MRI appeared to have healed (Figs. 4B and 5B). Follow-up radiographs at 9 months after injury showed mild joint space narrowing and a marginal osteophyte (Fig. 6). Union of the femoral head fracture was confirmed on 9-month follow-up CT scans. There was minimal flattening at the superior aspect of the femoral head, residual cortical depression, and small osteochondral loose bodies in the acetabular fossa and on the anterior aspect of the femoral neck (Fig. 7). 3D-CT reconstruction of the isolated right femoral head also showed step-off cortical depression and multiple loose bodies at the anterior aspect of the femoral neck. A final follow-up MRI conducted at 9 months after injury revealed a completely healed femoral head fracture (Figs. 4C and 5C).
During his final physical examination 9 months after injury, full range of motion of the affected hip was possible without pain or limping and he was not apprehensive about external rotation of the hip. The patient experienced no limitation regarding his military service. Furthermore, there was no evidence of avascular necrosis of the femoral head on MRI. No further treatment was planned because the small osteochondral loose bodies observed on CT scans were asymptomatic and were located in a non-weight bearing region.
DISCUSSION
Femoral head fractures occur in 5% to 15% of all hip dislocations. However, only 10 cases of femoral head fracture without hip dislocation have been reported, including ligamentum avulsion.1-3) Van der Werken and Blankensteijn2) first proposed that a fracture of the femoral head may precede its dislocation because forces are resisted by the firm superior portion of the acetabular rim with the hip joint in flexion of less than 60°. They suggested that direct blows to the greater trochanter in a relatively young person with normal bones may fail to break the neck of femur and instead transmit force to the femoral head. However, our patient fell on the ground with his right hip in flexion, external rotation, and abduction with knee extension and did not experience a direct blow to the hip joint.
Five of the 10 cases reported in the literature were documented as ligamentum avulsion fractures, in which relatively thin and small fracture fragments were attached to the ligamentum teres.4) In our case, MRI showed an undulating, elongated ligamentum teres with intrasubstantial edema and maintained continuity. Even if a small osteochondral fragment attached to the ligamentum teres adjacent to the fovea of the femoral head appeared to be avulsed by the ligamentum teres, the main fracture fragment was too large to have been caused by the avulsion force of the ligament. In addition, because a wedge-shaped osteochondral depression was present at the superomedial aspect of the femoral head, we presume that this fracture was caused not by direct blow to acetabular wall but by impaction of the acetabular rim. This fracture seemed to be analogous to Brumback type 4A, which involves an indentation type fracture and anterior hip dislocation.
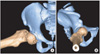
Our patient reported feeling that the right hip had been displaced from its joint for a moment. This probably represented subluxation with spontaneous relocation, and the hip might have subluxated anteriorly because it was in flexion, external rotation, and abduction during the fall. Pringle and Edwards5) in a cadaver study, suggested a mechanism of anterior dislocation achieved by abducting and externally rotating the hip. Flexion of the hip creates an inferior obturator dislocation, whereas extension creates a superior pubic dislocation. Extreme abduction causes the femoral neck to abut against the posterior margin of the acetabulum, which allows leverage forces to pull the femoral head out and in front of the acetabular cavity. The posterosuperior and lateral portions of the femoral head impinge against the anteroinferior margin of the acetabular rim to produce an impaction fracture of the femoral head and occasionally an osteochondral fracture of the anteroinferior margin of the acetabular rim.6) Indentation fractures of the femoral head are rare and have a poor long-term prognosis. All reported cases of indentation fractures have been attributed to high-energy trauma and treated by closed or open reduction. In these cases, fractures were located on the posterosuperior and lateral portions of the femoral head.7) However, in our case, the impacted fracture was caused by low-energy trauma and was presumably associated with subluxation or dislocation with spontaneous relocation. Prognosis was good with conservative treatment because the location of the fracture was medial of the weight-bearing portion. The direction of the impacted fracture on 3D reconstructed CT images differed from those of previously reported indentation fractures, from posterolateral to anteromedial (Fig. 8). The impacted fracture of this patient was probably produced by impingement of the femoral head against the anterior edge of the acetabular rim with the hip in abduction, external rotation, and flexion (Fig. 9). The possible mechanism of this fracture was simulated using 3D reconstructed CT images of this patient (Fig. 10).
To our knowledge, only 2 cases of anterior hip dislocation by low-energy trauma have been described in the literature. Stein et al.8) reported the case of a healthy young woman who sustained an anterior hip dislocation while participating in a noncontact activity (ballet dancing) and Ruppert9) reported a 46-year-old male patient without any prior deformities dislocated his right hip while playing soccer. However, in both cases, there was no associated femoral head fracture and dislocated hips were treated by closed or open reduction under general anesthesia, respectively.
Despite the small number of reported cases, it is known that recurrent dislocation of the hip may be influenced by predisposing factors such as connective-tissue disorders, dysplasia of the femoral head or acetabular rim, fractures, neural deficits, or labral or capsular ruptures.10) Trousdale10) reported a patient with recurrent anterior hip instability with excessive acetabular anteversion and multiple loose joints who was treated by periacetabular osteotomy. Our patient showed general ligament laxity during physical examination. However, there were no structural abnormalities of the femoral head or acetabulum and connective-tissue disorders were ruled out after a complete rheumatologic evaluation.
In conclusion, a CT scan or MRI should be performed to rule out a fracture of the femoral head if a patient is suspected to have dislocated or subluxated the hip after carefully reviewing the trauma history. A CT scan or MRI should be performed even after a low-energy injury incident without a definite bony abnormality in plain radiographs, especially in patients with general ligament laxity. In our case, despite roentgenographic evidence of minimal degenerative changes at his final follow-up visit, the clinical results of conservative treatment were better than those of other reported indentation fractures because the femoral head fracture was located medial to the center of the femoral head in a non-weight bearing region.







 XML Download
XML Download