

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Tendon-bone junctions are composed of a complex mix of hard bony and soft tendon tissues. The restoration of collagen fibers and fibrocartilage in the transitional zone after injury is crucial in terms of regaining the mechanical properties of the tendon-bone junction. However, this transitional region has poor healing potential due to its hypovascularity.1,2)
Previous studies have examined bone-tendon junction healing within bone tunnels, and various methods have been devised to improve early fixation and to facilitate healing. These methods have included decortication and the creation of a bone trough, the use of a dowel plug, and stapling.3-5) In the past, shock waves, allogenic chondrocytes, platelet-derived growth factor, and bone marrow matrix cells with bone morphogenetic protein have been reported to facilitate bone-tendon junction healing.6-10) However, few studies have been reported an accelerated healing of bone-tendon junction injuries.6,11) Platelet-rich plasma (PRP) has attracted much attention, because it is a safe and cost effective source of growth factors that stimulate cellular regeneration, and as a result, many reports have been issued on the osteogenic effect of PRP.12-16) In addition, PRP has been reported to accelerate tenocyte proliferation and collagen production by injured tenocytes.17) PRP from bone marrow aspirate contains platelets, growth factors, and condensed nucleated bone marrow cells, all of which contribute to tissue regeneration.18)
Repair processes after tissue injury are regulated by different cell types, growth factors, and proteins. Of these growth factors, bone morphogenetic protein (BMP) regulates cell proliferation, differentiation, apoptosis, morphogenesis, and organogenesis.19-21) Furthermore, experimental studies have revealed that BMP has a beneficial effect on tendon healing.19)
We hypothesized that PRPs could accelerate tendon healing and BMPs bone healing at the tendon-bone junction. The present study was designed to evaluate and to compare the microscopic features and mechanical properties of tissue healing in surgically created tendon Achillescalcaneus junction injuries in a rabbit model in response to exogenous BMP-2 plus bone marrow PRP in a fibringlue carrier.
METHODS
Animals
Three-month-old skeletally mature male New Zealand white rabbits (n = 54, 3.5 ± 0.5 kg; Jung-Ang Animal Laboratory, Seoul, Korea) were housed in cages and fed commercially available rabbit food. Right hind legs were used for the experiment and left hind legs were preserved. NIH guidelines for the care and use of laboratory animals published by the National Institute of Health (NIH publication no. 85-23, revised 1985) were observed throughout the study.
Preparation of Bone Marrow Derived PRP
The animals were anesthetized with an intramuscular injection of 250 mg ketamine hydrochloride (Yuhan, Seoul, Korea). Standard sterile drape was applied to the pelvic area, and 2 mL of bone marrow was aspirated in the standard manner from iliac crests. Autogenous PRP was obtained by centrifuging bone marrow aspirates at 4,000 rpm for 10 minutes.
Surgical Procedure
Under standard aseptic conditions, an L-shaped skin incision was made over the posterior aspect of the each right heel and the insertion site of the Achilles tendon was exposed. The tendon was transected at its insertion and a bone tunnel was made on both sides of the calcaneus using an arrow pointing device (towel clip). The tendon was reattached later at the calcaneal tuberosity using a pullout steel wire 2-0 suture (Ethicon, Johnson & Johnson International, Warsaw, IN, USA). The plantaris tendon also transected (Fig. 1).
The animals were divided into 3 groups: in the control group (n = 18), after reattaching the tendon, no further procedure was done; in the other second group (each n = 18), a mixture of bone marrow derived PRP and fibrin glue (0.1 mL; the PRP/fibrin group); and in a 3rd group, bone marrow derived PRP, BMP-2 (Sigma-Aldrich, St. Louis, MO, USA), and fibrin glue (0.1 mL of fibrin glue mixed with 100 ng/mL of BMP-2 and 0.05 mL of bone marrow derived PRP: the PRP/BMP-2/fibrin group) was injected into the tendon-bone repaired gap. Wounds were closed in a layered fashion and limbs were immobilized using a short leg cast in the position of ankle-plantar flexion. Rabbits were allowed to move freely within their cages. Six rabbits per group were sacrificed at 2, 4, and 8 weeks after surgery for evaluation.
Tissue Sample Preparation
Animals were anesthetized with an intramuscular injection of 250 mg ketamine hydrochloride and euthanized with i.v., potassium chloride. Under standard aseptic conditions, previous surgical wounds were opened and the tendon Achilles-calcaneus complex was harvested. Harvested specimens were examined grossly and findings were recorded. Specimens were allocated randomly for histological and mechanical studies.
The specimens for histological analysis were fixed in 10% buffered formalin, decalcified with decalcifying agent (Decal Rapid, National Diagnostics, Atlanta, GA, USA), dehydrated using a graded alcohol series and embedded in paraffin. Tissue sections (6 µm) were cut perpendicular to the tendon-to-bone junction and stained with H&E and Masson's trichrome. Specimens for biomechanical studies were frozen separately at -70℃ in 50 mL bottles until required for testing.
Histological Analysis
The following parameters were assessed using a light microscope (Zeiss, Carl Zeiss, Oberkochen, Germany): cell types, nature of the matrix present in the tendon-bone interface, collagen fiber alignment, amount of fibrocartilage, and new bone formation.
Mechanical Testing
Frozen specimens were thawed in normal saline at room temperature before testing, and the cross-sectional area of healing interfaces were measured. In each case, the tendon Achilles-calcaneus complex was securely fixed in a specially designed apparatus, which allowed the specimen to be oriented such that a tensile load could be applied along the axis of the tendon. The whole construct was loaded onto an Instron mechanical tester (Instron 4201, Instron, Canton, MA, USA) operated at 10 mm/minute velocity traction speed. Maximum strain, maximum load, ultimate stress, and elasticity modulus were recorded on a personal computer.
RESULTS
Gross Findings
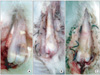
For all the specimens from each treatment group, the Achilles tendon was loosely connected to calcaneus bone and adhered to surrounding soft tissues. Few differences were observed between the groups at any time point (2, 4, or 8 weeks after surgery) (Fig. 2).
Histological Analysis
At 2 weeks after surgery, cartilage formation was observed at tendon-bone junctions in the control group. Fibrocartilage formation was observed at tendon-bone junctions in the PRP/fibrin and the PRP/BMP-2/fibrin groups, and woven bone was visible in the PRP/BMP-2/fibrin group (Fig. 3).
At 4 weeks, fibrocartilage was observed in the control group and woven bone in the PRP/fibrin group. Fibrous tissues in junctions were well aligned with bone in the PRP/BMP-2/fibrin group. At 8 weeks, fibrous tissues were loosely connected to bone in the control group, but fibrous tissues were connected to bone through newly formed cartilages in the PRP/fibrin group and to bone through new bones in the PRP/BMP-2/fibrin group (Fig. 4).
Mechanical Testing
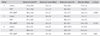
Mean maximum loads at failure of tendon bone junction complexes were 47.9 ± 24.9, 74.7 ± 18.6, 60.5 ± 15.0 N respectively in the control, the PRP/fibrin group, and the PRP/BMP-2/fibrin group for specimens obtained at 2 weeks after surgery. Mean maximal load at failure in the PRP/BMP-2/fibrin group was second highest, but this was not significant (p > 0.05). Corresponding mean maximum loads at failure at 4 weeks after surgery were 46.1 ± 4.3, 61.3 ± 28.5, 73.9 ± 19.5 N, again the mean maximal load at failure was not significantly greater for the PRP/BMP-2/fibrin group. Similarly, mean maximal loads at failure at 8 weeks were 62.4 ± 4.9, 89.8 ± 4.6, and 99.6 ± 10.3 N, respectively, but on this occasion the mean maximum load at failure was significantly greater in the PRP/BMP-2/fibrin group (p = 0.007) (Table 1).
DISCUSSION
The Achilles tendon-calcaneus bone complex in our study serves as a good model for bone-tendon junction injury. The healing of tendon-bone junction is restoring alignment of collagen fibers and fibrocartilages with appropriate mechanical strength at the transition zone after an injury. Restoration of collagens and fibrocartilages between tendon and bone is essential for regaining the mechanical properties of the bone-tendon junction.22) About 8 week is healing time of rabbit's tendon-bone injury, but the mechanical strength is up to 80% of normal tendon bone junction.23) In this study, improvement of biomechanical properties of scar tissue with time in all groups suggested that healing progressed with time. Fibrocartilage is one of the components of repaired tissue at tendon-bone junction injury. Thick fibrocartilage may reinforce the link of between tendon and bone.24) The direct insertion complex of tendon bone junction is transitionally composed of a tendon, onocalcified fibrocartilage, calcified cartilage, and bone. This four-zone arrangement yields a gradient of mechanical stiffness that avoids traumatic injury due to concentration of stress at interface.25) Histologically fibrocartilage formation was observed earlier in PRP/fibrin group and PRP/BMP-2/fibrin in our study. Tendon was connected to the calcaneus bone through the fibrocartilage and new bone in 8 weeks PRP/BMP-2/fibrin group specimens. We thought that bone marrow derived autogenous PRP and rhBMP-2 gave strong integration between Achilles tendon and calcaneus bone. In this study, we found that a mixture of bone marrow derived autogenous PRP, rhBMP-2, and fibrin glue connected tendons to bone through newly developed bone and promoted mechanical stability following repair of a ruptured tendon-bone junction. Mechanical stability increased significantly with time after injecting bone marrow derived autogenous PRP, rhBMP-2, and fibrin glue into ruptured sites.
PRP has been used as source of platelet derived growth factor and transforming growth factor,26) and it has been reported that PRP has a positive effect on cell proliferation and collagen production, and that it induces the production of matrix-degrading enzymes and endogenous growth factors by human tenocytes.17) Furthermore, some reports have shown that PRP has osteogenic effects.12,14-16) In particular, PRP derived from bone marrow contains growth factors and mesenchymal stem cells, and these cells have been reported to promote tendon injury healing.27)
BMP are bone forming factors and can accelerate bone formation in tendons.21) Cartilage-derived BMP has been reported to promote the formation of large, strong tendon calluses.26) Rodeo et al.,28) in a dog model, demonstrated that recombinant human BMP-2 accelerated tendon to bone healing in a bone tunnel and that it induced a transitory increase in pull-out strength. In a previous study, we found that BMP-2 accelerated the formation of fibrocartilage during the early phase of healing and increased the biomechanical strength of bone-tendon junctions.6) However, no report has been issued on the effect of bone marrow derived PRP mixed with BMP-2. In the present study, a mixture of bone marrow derived PRP and BMP-2 was found to promote the production of bony tissue tendon/bone junctions and to increase biomechanical strength.
Fibrin glue can be used as a carrier of exogenous cytokines and metabolized without foreign bodies,29) and thus, we used fibrin glue as a carrier in the present study.
In the field of orthopaedic surgery, there are many kinds of tendon bone junction injury such as rotator cuff tear, collateral ligament injury of knee, patellar tendon injury, Achilles tendon injury and extensor tendon injury of finger. Furthermore, the tendon reconstruction and tendon transfer is issue of the tendon bone integration. Autogenous PRP mixed with BMP-2 could give early stability to tendon-bone junction such as, rotator cuff repair, anterior cruciate ligament graft and tendon transfer around foot and ankle area in clinical situation from our study results.
In conclusion, bone marrow derived PRP plus BMP-2 was found to improve significantly the mechanical strength of tendon bone junctions and to accelerate the formation of fibrocartilage and new bone after tendon to bone junction injury.



 XML Download
XML Download