

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hamstring strain is caused a wide range of sporting activities with the vast majority of these injuries responding well to nonsurgical treatments. In contrast, a complete rupture of the proximal hamstring origin is rare and currently management varies from conservative treatment in a flexion splint to acute or delayed surgical repair. Reports of surgical treatment of a proximal hamstring rupture are few and contain relatively small numbers of both acute and chronic tears.
In 1988, Ishikawa et al.1) reported two cases of proximal hamstring avulsions from ischial tuberosity. Both patients underwent surgical repair (one patient 5 days and the other, 2 months after injury) with good functional results. Orava and Kujala2) reported eight patients treated surgically for proximal hamstring tendon ruptures. Four patients were operated on during the acute phase of the injury, whereas the other four patients underwent surgery at least 2 months after the injury. The authors concluded that surgery should be performed promptly within the first few days after the injury. If surgical repair is delayed, it is not possible to accomplish a primary suture of the hamstring muscles to the ischial bone and another surgical procedure will be needed to restore function. Klingele and Sallay3) reported the surgical repair of complete proximal hamstring tendon ruptures in eleven patients. The repairs were performed for seven acute injuries and four chronic injuries. Acute repairs were defined as those repaired less than 4 weeks after the injury. Brucker and Imhoff4) published a functional assessment after the surgical treatment of acute and chronic complete ruptures of the proximal hamstring tendons in eight patients. Six patients underwent surgery within 3 weeks after the trauma, whereas two patients underwent surgery after a delayed diagnosis of more than 2 months. The authors recommended early surgical repair using a bone-anchor-suture-tendon system and protective bracing for post-operative 6 weeks in both acute and chronic cases. In 2008, two reports of a larger series of proximal hamstring ruptures were published by Sarimo et al.5) (14 acute and 27 chronic case) and Folsom and Larson6) (21 acute and 5 chronic cases), who concluded that acute surgical repair of proximal hamstring ruptures is easier to perform, provides better results and high return to the preinjury activity level than late surgery and is therefore recommended. The present paper reports two cases of acute complete rupture of the proximal hamstring tendons that were treated successfully with early surgical repair.
CASE REPORTS
Case 1
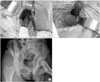
A 24-year-old male professional football player sustained an injury during a football game. The patient noticed sharp pop with accompanying severe pain in the right buttock and proximal posterior thigh when he attempted to kick a ball up hard. The clinical signs included swelling and ecchymosis on the proximal posterior thigh, tenderness to palpation at the ischium, and weakness with active-resisted knee flexion. A palpable defect was not obvious because the injured site was swollen considerably by the hematoma (Fig. 1). There was no X-ray evidence of a fracture of the ischium and magnetic resonance imaging scans (MRI) revealed a complete proximal hamstring rupture at the level of the ischial tuberosity (Fig. 2). The patient was operated on 6 days after the injury. The patient was placed in the prone position and a 15 cm vertical incision was made to the posterior proximal thigh starting at the gluteal crease and continuing distally. The avulsed hamstring tendons were exposed easily by dividing the posterior fascia and retracting the gluteus maximus superiorly. The posterior cutaneous femoral and sciatic nerves were exposed and spared. A single tendon comprised of all three tendons (Fig. 3A). The lateral side of the ischial tuberosity was cleared off using a curette to induce healing of the torn tendon to the bone, and three FiberWire No. 2 suture anchors (Arthrex, Naples, FL, USA) were placed in the exposed ischium. To place sutures under sufficient tension, one limb of each suture was woven into the tendon using a crisscross stitch while the other limb was placed on a simple suture to pull the tendon (Fig. 3B-C). The knee flexion > 30° was maintained when the sutures were tied down. After closing the surgical wound, the operated limb was placed in a hip-knee-foot orthosis with the hip in the neutral position and the knee in 60° flexion to relax the repaired tendon.
The patient was instructed to avoid sitting for the first 2 weeks. After 2 weeks, the brace was opened gradually for range of motion exercises but the patient was instructed to refrain from simultaneous hip flexion-knee extension. The brace was discontinued after 2 months and gradual strengthening exercise was started. Partial weight bearing exercises and full weight bearing were allowed after 6 weeks and 3 months, respectively. Six months after surgery, the patient had a full range of motion at the hip and knee joints and could resume their near normal activity of daily living. Sports activity was allowed after 8 months and the patient could return to his pre-injury level of sport without apparent limitations or pain at a final follow-up of one year after surgery.
Case 2
A 16-year-old man was given a kick on the anterior side of the left distal thigh by his opponent while practicing Taekwondo. At that moment, his left hip joint flexed abruptly while his left knee was forcibly extended by the kick. Simultaneously, he noticed sudden pop and severe pain in the proximal posterior left thigh. X-rays showed no abnormality of the left ischial tuberosity but the MRI revealed a complete proximal hamstring rupture at the level of the ischial tuberosity (Fig. 4). The patient underwent surgery on 5 days after the injury. The patient's leg was operated and rehabilitated in the same manner as described for case 1.
Six months after surgery, he had a full range of motion of the hip and knee, and was asymptomatic with his daily activities. However, one year after surgery, he had not been able to return to practicing Taekwondo due to a fear of reinjury.
DISCUSSION
Complete rupture of the proximal hamstring origin normally arises from a violent overstretching of the contracted hamstring muscles while the hip is flexed and the knee is extended. Reports of surgical treatment of a proximal hamstring rupture are few, include relatively small number of patients, and contain both acute and chronic tears. Often there is a considerable delay in diagnosis because of its rarity, difficulty in clinical diagnosis by deep seating of the injured tendons beneath the thick layer of adipose tissue and the belly of the gluteus maximus muscle, initial attempt of conservative care, and under-appreciation of the residual loss of function in non-surgically treated cases. MRI is essential for a correct diagnosis in cases where a tear is suspected.3,5,7-9)
Interest in the surgical treatment of these injuries has increased as poor functional results have been reported among patients treated non-surgically.4,6,7,9,10) Sally et al.10) reported the functional outcomes of 12 patients who had hamstring injuries (six complete and the other six partial) and treated initially non surgically. Six patients who sustained partial tears could return to most of their preinjury sports but five patients, all with complete tears, were unable to run or participate in any sports requiring agility. Only one female patient with a complete tear was satisfied with her function.
Recently, many authors reported that early surgical repair of complete proximal hamstring ruptures, which is defined as those repaired less than 4 weeks after the injury, produced better results and a high return to full activity than late surgery.3-6) Folsom and Larson6) reported excellent results with a high return to full activity in 21 acute and 5 chronic injuries treated surgically. They suggested early repair for active patients to allow easier repair and an early return to function. Sarimo et al.5) reported the surgical treatment of complete proximal hamstring tendon ruptures in 41 patients. When the patients were divided into 3 groups (0-3 months, 3-6 months, and > 6 months) according to the delay from injury to surgery, there were significant diff erences in the result. According to the results, they concluded that early surgical treatment produces better results than late surgery and is therefore recommended.
The surgical techniques advocated most frequently for acute repair of complete ruptures of the proximal hamstring tendons include transosseous fixation methods using multiple drill holes in the ischium or a bone-anchorsuture-tendon system.1,2,5,6)
In chronic cases, the anatomical reattachment of torn tendons is much more difficult than acute cases and often the knee has to be flexed and immobilized more to achieve apposition and reduce the tension on the repaired tendons until complete healing. Many authors deem extensile exposure necessary to identify scarred, retracted muscles in chronic cases. In addition, the sciatic nerve is frequently encased in scar tissue and requires neurolysis, which poses a risk to the nerve branches. Proximal tendinous tissue is normally tenuous as the torn tendons were successfully mobilized to the ischium and call for additional augmentation. When it is impossible to pull the torn tendons back to the ischial tuberosity, various types of reconstructions are needed to bridge the torn end to the ischial tuberosity.5,6,9,10) Based on the literature available and our own experience, it is believed that acute injuries are easy to repair, and early repair yields excellent functional results. Furthermore, the surgeon can avoid the problems of chronic scarring in delayed repair.
Postoperatively, immobilization of the knee at a considerable degree of flexion and hip in neutral position with orthosis lasting for 4 to 6 weeks has been recommended to avoid stress on the repaired hamstrings.2-4,8) Folsom and Larson6) found it unnecessary to restrict the hip range of motion when knee motion is controlled and used a standard hinged knee brace instead of a hip/knee orthosis. After 2 to 6 weeks, the brace was opened gradually and range of motion exercises combined with isometric exercises were started. After the brace was discontinued at postoperative 6 to 8 weeks, the patient was allowed to bear weight where tolerated. Overstretching of the hamstrings must be avoided for the first 4 weeks and simultaneous hip flexionknee extension is not allowed for 2 months after surgery. More intensive physical therapy with special regard to stretching and strengthening of the hamstrings, should begin at 2 to 4 months, and sports activities be allowed 6 months after surgery depending on the type of sports and the patient's progress. The two patients in this report underwent a postoperative physical therapy regimen based on the protocol above.
A complete proximal hamstring rupture is a serious injury that can lead to significant disability. The authors believe that early surgical repair is recommended for young, active male and female patients because non-surgical treatment result in complications, such as muscle weakness including a sense of poor leg control, sciatic neuralgia, and distal bulge caused by the retracted muscles. For female patients, a transverse incision in the gluteal crease is recommended when cosmetic problems are considered. These injuries might be more common than previously appreciated. We believe that a high clinical suspicion of the examiner based on the reported mechanism and clinical findings, and the prescription of a MRI scan in cases where a tear is suspected would reveal the injury in the early stage and make acute repair possible.



 XML Download
XML Download