

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Surgical treatment is the best option for managing intertrochanteric fractures.1,2) Of the many methods used, the gold standard is closed reduction and internal fixation by any means. To obtain the best clinical outcome, most reports agree that an anatomic reduction3,4) followed by rigid fixation without a device allowing controlled impaction is important.2,5) Nevertheless, this simple strategy is sometimes difficult, particularly when an unstable or even irreducible fracture is encountered. Some of these difficult fractures had sagittal displacement that could not be reduced closely. In such cases, the fracture may appear to be reduced in an anteroposterior radiograph after traction and internal rotation. However, when the lateral image was checked, it showed marked displacement in the sagittal plane. Among these cases, we identified a specific type of fracture that cannot be reduced under usual traction, rotation and elevation of distal thigh. Although this might not be new, this fracture pattern can be called a "sagittally unstable fracture." For this case, an open reduction was attempted with a bone clamp followed by fixation with or without additional circlage wires. This procedure requires relatively large surgical exposure and a long anesthetic time, which can potentially bring delayed rehabilitation or wound problems. Therefore, a search was made for more simple and less invasive methods for reduction. After several trials and errors, a relatively simple method was found to reduce the anterior and medial cortices of the fracture using one or two Steinman pins as a joystick. This report introduces this simple technique and its results after a 1-year-follow-up.
METHODS
Definition of the Fracture
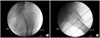
Among the fracture patterns from the AO/ASIF classification, 31 A1.3 to 31 A2.3, a specific fracture pattern that could not be reduced easily on the sagittal plane was found. This contains the one in which the oblique fracture surface of the distal fragment in the lateral radiographs faces anterosuperiorly, so that the distal shaft fragment falls in the posterior direction when the patient is laying on the fracture table. When traction is applied to this fracture, the proximal fragment is usually flexed and the shaft fragment falls posteriorly. This displacement could not be corrected, even after elevation of distal thigh with external support. This condition can be worsened if the proximal fragment has a long medial beak or a part of the intact lesser trochanter on it (Fig. 1).
Surgical Technique
When this fracture pattern was noticed during an initial effort at reduction under fluoroscopic guidance, an attempt was tried to obtain rotational alignment only regardless of the displacement on the other plane. If satisfactory rotational alignment was obtained, the patient was prepared and draped. Surgery was performed by an operator and one assistant. The assistant elevated the patient's thigh with a mallet placed vertically on the arm of the fracture table. A 4.2 mm Steinmann pin was introduced through a 2 mm stab wound made at the cross section of an imaginary vertical line drawn from the anterior superior iliac spine and a horizontal line at the level of the tip of the greater trochanter (Fig. 2). The tip of the Steinmann pin was placed at the inferomedial cortex of the proximal fragment in the anteroposterior (AP) radiograph and at the anterior cortex of the proximal fragment in the lateral image. With the pin, the operator pushed the anterior cortex downward and simultaneously levered the medial cortex laterally to reduce both the anterior and medial cortices (Fig. 3). Keeping the pin in situ, the fracture was fixed using the Proximal Femoral Nail Antirotation™ device (PFNA; Synthes GmbH, Solothurn, Switzerland). The Steinmann pin should be placed on the cortex, so that it would not interfere with the installation of an implant. Because maintaining the reduction is necessary only for a short period while installing a helical blade, the operator could control both the pin and instrument without difficulty.
A two-pin-technique was used if satisfactory rotational alignment could not be obtained during the initial closed reduction. First, one 3.5 mm Steinmann pin was introduced through the same entry portal described above. The tip of the pin was placed 1-2 cm proximal to the center of the fracture line at the proximal fragment. After rolling and tapping it to pass through both cortices, the proximal fragment was rotated using that pin as a joystick. Instead of drilling, rolling and tapping the pin was chosen to penetrate the cortex to avoid possible tissue damage while drilling the pin through a small opening. After confirming the rotational alignment, the second pin (4.2 mm S-pin) was then placed and controlled using the same technique described in the previous paragraph. Because the first pin could be in the path of the helical blade, it was removed after the guide wire for the helical blade was successfully installed, while the second pin was kept in situ until the end of the procedure (Fig. 4).
Patients
One hundred and nineteen low-energy intertrochanteric fractures in 115 patients aged were 65 years or older underwent surgery from January 2007 to December 2008. Of them, 21 hips in 20 patients had this fracture pattern. Although the degree of displacement varied, it was confirmed that simple longitudinal traction with slight internal or external rotation made the fracture geometry worse. In all cases, the fracture was reduced using the percutaneous reduction technique. Of them, 19 hips in 18 patients were followed up for at least one year (one patient died and one was lost to follow-up). The mean age of the patients was 77 years (range, 65 to 88 years). Fifteen patients were women and three were men. No additional methods were used for fixation including wires or screws. These patients were enrolled in the study group and the remaining 82 cases (79 patients; 10 died and six lost to follow-up), who did not show sagittal instability, were enrolled in the control group.
Assessment Method
The clinical assessment included the underlying medical illnesses, delay until surgery, anesthetic time, calculated hemoglobin loss during surgery,6) functional evaluation using the modified index of Koval et al.7) and postoperative clinical complications. The calculated hemoglobin loss was obtained by subtracting the serum hemoglobin concentration tested at least 24 hours after surgery from that obtained just before the surgery. Because one unit of a packed-cell-transfusion is known to elevate the serum hemoglobin by 1 g/dL,8) the number of units transfused during this period, if any, was added to the hemoglobin loss. The radiographic assessment included the adequacy of the reduction using a modification of Baumgaertner's classification by Fogagnolo et al.,9) change in the neck-shaft angle, amount of sliding of the lag-blade, medial displacement of the femoral shaft , and radiological complications. All radiographic data were corrected for the degree of magnification using the known diameter of the lag blade.
RESULTS
The mean age and number of medical illnesses of the patients in study group was 77 (range, 65 to 88) and 1.4 (range, 0 to 3), respectively. The most common medical illness was diabetes. Recent (within 1 year) cerebrovascular disease was noted in six patients. The mean time delay before surgery was 2.8 days (range, 1 to 6 days). According to the AO classification, six, seven, and six patients in the study group were classified as A1.3, A2.1, and A2.2 or more, respectively. The gender and age distribution, number of comorbidities, and incidence of recent (within 1 year) cerebrovascular disease were similar in both groups. The mean time delay before surgery was also the same. The fracture stability measured using the AO classification was similar in both groups. The mean pre-injury activity level of the patients and mean activity level at the final visit was significantly lower in the study group than that of the control group (p < 0.01). On the other hand, the mean degree of recovery after surgery (the difference between the activity level before and after treatment) was the same (p = 0.34). The mean calculated hemoglobin loss during surgery, incidence of transfusion and the total anesthetic time were similar in the two groups. No clinical complications attributed to this technique, such as wound problems, inadvertent neurovascular injury, tissue damage or infection, were encountered. The clinical results are summarized in Table 1.
Radiologically, satisfactory reduction (good or acceptable) was obtained in all cases. The change in neck-shaft angle (p = 0.06), amount of sliding of the lag blade (p = 0.64), amount of medial displacement of the femoral shaft (p = 0.07), and tip-apex distance (p = 0.06) was similar in the two groups. Although the incidence itself was similar, no case of cutout was observed in the study group, whereas two occurred in the control group (p = 1.00). Union was achieved in all but two hips with cutout. The mean time for radiological union was similar in the two groups (p = 0.56). There were no radiological complications that were related to this technique. Table 2 summarizes the radiographic results.
DISCUSSION
Although two earlier classification systems have been introduced,10,11) most studies focused on the anteroposterior image of the fractured hip.12) Almost all fractures can be categorized successfully using these classifications but they are not always perfect. Fracture patterns that do not easily fit any classification system can be identified easily. Some cannot be reduced closely during surgery. A few reports on these unusual fracture patterns referred to them as "irreducible fractures" and recommended open reduction.13,14) Some difficult fractures were also experienced by the authors. Among them, a specific pattern in the sagittal plane regardless of the coronal plane geometry was noted. If the oblique fracture surface of the distal fragment faces posteriorly, the sagittal geometry usually can be reduced after traction and rotation with the help of gravity. In contrast, if the oblique surface faces anteriorly, the traction maneuver results in posterior sagging of the shaft fragment and anterior angulation of the proximal fragment. The sagging can be restored if the thigh is elevated with external support but the anterior angulation of the proximal fragment cannot be reduced. This phenomenon worsens if the proximal fragment has a long medial beak or includes a part of the lesser trochanter. In those cases, an intact psoas tendon may intervene between the fragments or pull the fragment directly so that it makes the closed reduction almost impossible. Many surgeons have already noted this type of difficult fracture and suggested surgical tips to reduce them, including the use of crutches15) but there has not been any clinical series that dealt with this sagittal instability.
The key factors for the successful treatment of hip fractures in the elderly are reducing the surgical invasiveness for treatment, obtaining stable geometry and rigid internal fixation, and encouraging early mobilization. To achieve these goals, the proximal intramedullary nail was chosen as a fixative method. Placing a nail in a sagittally unstable intertrochanteric fracture can often aggravate the reduction and result in an unsatisfactory geometry. Few reports have offered surgical tips to reduce these difficult fractures. Most adopted the concept of elevating the distal shaft and direct compression of the proximal fragment.5,16) We completely agree with the basic concept of these techniques. After several trial and error series, the fracture could be reduced using S-pins inserted percutaneously. During surgery, an assistant sits beside the fracture table and holds the mallet with both hands to elevate the thigh. Manipulating the pin is required only for a short period while installing a helical blade. Therefore, the operator can handle both the S-pin and instrument for inserting a helical blade when necessary. In all cases, only one additional stab incision was necessary. The entry point for the S-pin was determined by the same manner as commonly used in hip arthroscopy.17) In addition to the downward push, some lateral hooking force was also needed in most cases. Reduction was achieved in 16 cases in whom satisfactory rotational reduction was obtained before draping. Two-pin technique was necessary in two cases that the proximal fragments were displaced in a fixed position with severe external rotation. Although the fracture pattern was difficult, no additional time was needed for these specific techniques because the time could be reduced by avoiding repeated trials and hesitation for closed reduction.
The mean activity level of the patients before injury was significantly lower in the study group than that of the control group. Since every possible condition that can affect the general health of the patients was not examined, it is unclear if this fracture always occurs in less mobile patients. On the other hand, the level of recovered activity was similar in the two groups after surgery. Using this technique, satisfactory reduction of this difficult fracture could be achieved, and maintained it until definitive fixation is completed. Initially, there was some concern regarding the potential problems with this technique, such as wound maceration, lateral femoral cutaneous nerve injury, inadvertent vascular puncture, complications related to the increased surgical time or adding comminution. Nevertheless, no complications related to this procedure were encountered. Iatrogenic comminution can be avoided by exact pin placement and traction. An attempt should be made to locate the tip of the pin at the anteromedial cortex, which is believed to be the strongest part in the proximal fragment. Moreover, the remaining capsule in this area could prevent the pin from slipping during manipulation. In addition, sufficient traction was used just before manipulation to provide sufficient space for the reduction; it was released after obtaining satisfactory reduction.
Since this study was not prospective or randomized, the results cannot be considered conclusive. Furthermore, too few patients were involved. A comparison of the result between these two groups was not reasonable because the basic fracture pattern was different. The best scientific conclusion would have been derived if the result of open reduction and percutaneous reduction to the same fracture geometry were compared but such study design would be unethical because an open reduction with wide exposure in elderly patients could do more harm than this simple technique. Despite these weak points, this study provided several informative results. This technique was performed only in highly selected cases with the same difficult fracture geometry and the results were compared with simple and the usual cases fixed with the same devices. Since this percutaneous technique was not used in the control group, the only difference in the treatment of the two groups was the reduction technique. By adding this simple technique, it may be possible to treat a difficult fracture in the same way as simple and reducible fractures.
In conclusion, if one encounters this fracture pattern in practice, do not spend time on repeated attempts for closed reduction. Just drape the patient in situ, elevate the leg with any device, and push down or rotate the proximal fragment using S-pins as a joystick. This simple percutaneous technique can help the surgeon achieve satisfactory reduction in sagittally unstable intertrochanteric fractures.




 XML Download
XML Download