

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Because the posterior horn is relatively immobile compared to other parts of the medial meniscus, it is vulnerable to tears.1) Recently, radial tears of the medial meniscus posterior horn have become increasingly recognized.2-4) Ozkoc et al.4) reported that this type of meniscal tear is strongly associated with obesity and older age, and is usually accompanied by degenerative chondral damage in the compartment involved. Horizontal tears are known as degenerative tears and are more common in the elderly population.5)
Although radial tears of the medial meniscus posterior horn and horizontal tears are similar in that both tears are degenerative tears and commonly occur at the posterior horn of the medial meniscus, the morphology of these two tears is quite different. Recently, many reports on the clinical features of radial tears of the medial meniscus posterior horn have been published but a comparison with other types of tears was not presented.2-4)
This study compared the clinical and radiologic features of radial tears of the medial meniscus posterior horn with those of horizontal tears.
METHODS
A retrospective review was performed on 387 patients (radial tears, 91 cases/23.5%; horizontal tears, 95 cases/24.6%; complex tears, 144 cases/37.2%; longitudinal tears, 57 cases/14.7%) who underwent arthroscopic treatment for medial meniscal tears by a senior author from January 2007 and December 2008. Among these, 186 cases (48.1%) with radial tears of the medial meniscus posterior horn and horizontal tears in the posterior segment of the medial meniscus were reviewed. Cases with complex tears and longitudinal tears were excluded. Complex tears were considered as all tears containing elements of at least 2 other types of meniscus tears. Patients with ligament laxity or prior meniscal surgery were also excluded.
Specific patient factors evaluated for the association with meniscal tear patterns included the patients' age, gender, duration of symptoms, body mass index (BMI) and injury history. The BMI was classified according to previously described criteria6,7) and the following scores: under weight, less than 18.5; normal weight, 18.5 to 24.9; overweight, 25 to 29.9; obese, 30 to 39.9; and morbidly obese, 40 or higher.
All patients underwent preoperative weight bearing anteroposterior and lateral radiographs. Each radiograph was graded from 0 to 4 for osteoarthritis using the original criteria of Kellgren and Lawrence8) as follows: zero, no degenerative changes; 1, questionable osteophytes and no joint space narrowing; 2, definite osteophytes with possible joint space narrowing; 3, definite joint space narrowing with moderate multiple osteophytes and some sclerosis; and 4, severe joint space narrowing with cysts, osteophytes, and sclerosis. The posterior slope of the tibial plateau was measured from the lateral radiographs. The anatomic femorotibial angle was measured from the weight bearing anteroposterior radiographs.
The indications for surgery were that the mechanical meniscal pain was more dominant than the arthritis symptoms and the meniscal signs (McMurray test and joint line tenderness) were clear. At the time of surgery, each patient underwent diagnostic arthroscopy to document the tear pattern and associated pathology. Chondral lesions involving the medial femoral condyle were classified into four different grades according to the Outerbridge classification.9) In many cases, more severe chondral lesions were inspected at the medial femoral condyle, so the medial femoral condyle was selected as the main lesions. At the time of arthroscopy, a 5-mm graduated probe was used to assess the size of each lesion. At least 2 crossed diagonal measurements were used. The Outerbridge classification was used to evaluate the severity of the cartilage lesions. For this study, the Outerbridge classification was defined as follows: grade 0, normal cartilage; grade I, cartilage with softening and swelling; grade II, a partial-thickness defect with fissures on the surface that do not reach the subchondral bone or exceed 1.5 cm in diameter; grade III, fissuring to the level of the subchondral bone in an area with a diameter > 1.5 cm; and grade IV, exposed subchondral bone.
A chi-square test was used to analyze the nonmetric variables in the form of frequency tables. The metric variables were tested using an independent sample t-test. Statistical analysis was performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA). A p-value < 0.05 was considered significant.
RESULTS
Patient Demographics
There were 143 females and 43 males. The average age of the patients was 56.4 years (range, 34 to 74 years). The mean duration of symptoms was 14 months (range, 1 to 120 months). Sixty-six cases (35.5%) had trivial injuries and 120 cases (64.5%) lacked an injury history. Ninety-one (48.9%) were radial tears in the medial meniscus posterior horn, and 95 (51.1%) were horizontal tears in the posterior segment of the medial meniscus.
Patient Demographics vs. Tear Shape
Age: The mean age of the patients with radial and horizontal tears was 57.6 ± 6.3 years and 55.2 ± 7.8 years, respectively. The difference was statistically significant (p = 0.024).
Gender: Of the 143 female patients, eighty (56%) had radial tears in the medial meniscus posterior horn, and 63 (44%) had horizontal tears in the posterior segment of the medial meniscus. In the 43 male patients, eleven (26%) had radial tears in the medial meniscus posterior horn, and 32 (74%) had horizontal tears. The incidence of radial tears was significantly higher in females than males (p < 0.001).
Duration of symptoms: The mean duration of patients with radial tears was 16.0 ± 22.3 months and the mean duration of patients with horizontal tears was 12.1 ± 16.0 months. This difference was not significant (p = 0.171). The duration of symptoms was divided into two groups: symptoms for less than 6 months (acute) and symptoms for more than 6 months (chronic). Forty-eight percent of patients with an acute presentation had a radial tear, compared to 50% of patients with chronic presentation (p = 0.776).
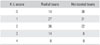
BMI: The mean BMI of the patients with radial and horizontal tears was 25.0 ± 2.7 and 24.3 ± 3.0, respectively. The difference was not significant (p = 0.084). However, there was a significant difference in the frequency distribution of BMI between radial tear and horizontal tear (p = 0.007). Table 1 summarizes the frequency distribution of the BMI according to the type of tear. There was a tendency for a radial tear to increase in the high BMI patients group.
Injury history: Of the 48 patients with an injury history, twenty-two (45.8%) were radial tears in the medial meniscus posterior horn, and 26 (54.2%) were horizontal tears. Of the 138 patients without an injury history, 70 (50.7%) were radial tears in the medial meniscus posterior horn, and 68 (49.3%) were horizontal tears. Forty-five percent of patients with an injury history had a radial tear compared to 51% of patients without injury history (p = 0.483).
Radiographic Findings
Kellgren and Lawrence radiographic score: The difference in the frequency distribution of the Kellgren and Lawrence (K-L) score between radial and horizontal tears was significant (p = 0.001). Table 2 lists the frequency distribution of the K-L score according to the type of tear. There was a higher tendency of radial tears in the high K-L score patients group.
Femorotibial angle: The mean angle of the patients with radial and tears horizontal was 1.5 ± 2.4° of valgus and 2.6 ± 2.5° of valgus, respectively. The difference was significant (p = 0.002).
Posterior tibial slope: The mean slope of the patients with radial and horizontal tears was 10.5 ± 2.9° and 9.3 ± 3.4°, respectively. The difference was significant (p = 0.014).
Chondral Lesions
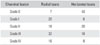
The difference in the frequency distribution of the severity of chondral lesions between radial and horizontal tears was significant (p < 0.001). Table 3 lists the frequency distribution of chondral lesions according to the type of tear. Of the 74 Outerbridge grade III or IV patients, 48 cases had radial tears in the medial meniscus posterior horn, and 26 cases had horizontal tears. There was a higher tendency of radial tears in severe chondral lesions.
DISCUSSION
Radial and horizontal tears are degenerative meniscal tears presenting in old age.2,4,5) Ozkoc et al.4) reported that 80% of patients with radial tears were older than 50 years with a female predominance. Bin et al.2) reported that most patients were older than 50 years, and 82% were female. In the above-mentioned studies, radial tears were not compared with other meniscal injuries. Therefore, they could not say that older age and a female predominance were unique features of radial tears. In this study, more radial tears were found in older patients than horizontal tears, and female patients predominated. Because the difference in the mean age of the two meniscal tears was not so great, older age may not be a unique feature of radial tears compared to horizontal tears. These results are in agreement with previous studies in terms of a female predominance, whereas older age was not a unique feature of radial tears compared to horizontal tears.
Osteoarthritis is a common condition related to overweight and obesity.10) Ford et al.11) reported a dose-response relationship between the BMI and meniscal surgery in middle-aged to older adults in both genders. Obesity is believed to increase the subchondral bony stiffness, transmitting more force to the overlying cartilage, suggesting a possible injury mechanism involving obesity.12,13) The menisci are believed to transmit more than half of the load to the knee joint.14) Therefore, there is a biomechanical mechanism for the relationship between BMI and meniscal tears. As the BMI increases, the torque in the knee joint during rotation likely increases, in theory leading to a higher risk of meniscal injuries. Ozkoc et al.4) reported that radial tears of the medial meniscus are closely related to obesity. However, they could not conclude that obesity is a unique feature of radial tears because they did not compare the BMI of patients with radial tears with that of patients with other meniscal tears. In this study, the mean BMI of patients with radial tears was larger than that of patients with horizontal tears but this difference was not significant. The ratio of obese patients in the radial tear group was higher than that in the horizontal tear group. Arthritis has been associated with obesity.12,13) In the present study, the arthritic changes in the radial tear group was more severe than in the horizontal tear group. This suggests that either obesity contributes to radial tears, or results from the radial tear and associated osteoarthritic changes.
Previous research demonstrated that increasing the tibial slope can cause a significant anterior shift of the tibia with respect to the femur.15) This anterior tibial shift may allow the posterior horn of the medial meniscus to become wedged between the femur and tibia and be torn more easily. In this study, the mean slope of the patients with radial tears was larger than that of patients with horizontal tears. This might explain the relationship between the tibial slope and radial tears.
Radial tears of the medial meniscus posterior horn were associated with severity of the chondral lesion and arthritic changes according to the K-L radiographic score. A biomechanical study reported that a posterior root tear of the medial meniscus caused a 25% increase in peak contact pressure compared to that found in the intact condition.16) Ozkoc et al.4) suggested that radial tears in the root of the posterior horn of the medial meniscus are usually accompanied by chondral damage. Horizontal tears generally do not disrupt the functional continuity of the circumferential fibers, and the meniscal functions were largely preserved.17,18) Christoforakis et al.5) reported that complex and horizontal tears are associated with the severity of cartilage degeneration compared to other types of meniscal tears. In that study, the mean age of the patients with other types of meniscal tears was 33.6 years. A limitation of this study was that only the severity of the most significant chondral lesions was evaluated according to Outerbridge classification and accurate anatomic maps of the chondral lesions could not be obtained. Nevertheless, these results suggest that radial tears may have more deleterious effects on the articular cartilage than horizontal tears.
Allaire et al.16) reported that radial tears caused a significant increase in varus alignment compared to that associated with an intact meniscus. They explained that lateral translation in combination with the loss of a spacer on the medial side of the knee allows compression of the medial compartment, resulting in varus alignment. These results are consistent with previous reports but the varus alignment might be a secondary result of degenerative arthritis.
In conclusion, radial tears of the medial meniscus posterior horn are a unique clinical entity associated with older age, females and obesity, and an increased incidence and severity of cartilage degeneration compared to horizontal tears.

 XML Download
XML Download