

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Triplane fractures are relatively rare fractures of the distal tibia that occur during closure of the distal tibial physis in adolescents. Since Marmor1) reported a triplane fracture consisting of three bone fragments in 1970, many authors have reported different types of triplane fractures categorized according to the number of fragments into those with two, three, and four main fragments. Some authors believed that different injury mechanisms will result in different types of triplane fractures. However, von Laer2) suggested that the level of the maturity of the physeal plate3) was a contributing factor.
Triplane fractures are difficult to examine using an anatomic approach due to their rarity and age-relatedness. In addition, the existence of different types of fractures makes it difficult to assess the precise fracture configuration form the plain radiographs. Accordingly, a correct anatomic reduction is difficult to achieve, and complications, such as premature closure of the growth plate and traumatic arthritis, can occur when an intraarticular fracture combined with growth plate damage is not treated properly.
The aim of this study was to identify the fracture con figurations of triplane and Tillaux fractures using computed tomography (CT) and assess the treatment outcomes.
METHODS
Materials
This retrospective study involved 14 patients (14 cases) who were available for a more than 1 year follow-up after treatments for a triplane and Tillaux fracture at our institution between July 1997 and June 2006. their medical records and radiographs were reviewed for the assessment. the mean follow-up period was 24.5 months (range, 12 to 108 months).
There were 12 males and 2 females with an average age of 13.9 years (range, 10 to 16 years). The injury mechanism included a sports injury in 5 cases, loss of footing in 5 cases, traffic accident in 2 cases, and fall from a height in 2 cases. At the time of the injury, there were 11 closed fractures and 3 open fractures.
Methods
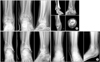
The plain radiographs and CT scan images obtained at the time of the injury were used to assess the fracture pattern. the cases involved were subdivided into the two and three part triplane fractures according to the number fragments and into the medial and lateral triplane fractures in accordance with the location of the displaced fragment (Fig. 1).4,5) The tibial fracture lines were observed on the anteroposterior and lateral radiographs to identify the presence of a tibial fracture and the association between the triplane fracture and external rotation force. Based on the injury mechanism, a closed reduction was achieved with adduction in cases of a medial triplane fracture and with internal rotation in cases of a lateral triplane fracture, respectively. To avoid an improper reduction, additional soft tissue damage and blood circulation disturbance, all procedures were carried out under general anesthesia. Screw or percutaneous Kirschner wire fixation was performed when satisfactory reduction was obtained. In situ fixation without reduction was not performed in any of the cases. An open reduction was performed in cases of an open fracture when more than 2 mm displacement after a closed reduction was observed. In cases combined with a tibial fracture, a reduction or internal fixation of the tibia was followed by an open reduction using an anteromedial approach for the medial triplane fracture and an anterolateral approach for the lateral triplane fracture, respectively. Fracture union, presence of a deformity, premature closure of the growth plate, and posttraumatic arthritis were assessed on the plain radiographs taken at the last follow-up to identify any complications. The treatment outcomes were evaluated using a modified Weber protocol. The outcomes were rated as excellent, good, fair, and poor based on the protocol for assessing pain, ambulation, activity, radiological outcome, foot function, and deformity.
RESULTS
Of the 14 cases, there were 3 cases of a Tillaux fracture and 11 cases of a triplane fracture. Of the triplane fractures, there were 7 cases with a two part triplane fracture and 4 cases with a three part triplane fracture. According to the location of the displaced bone fragment, there were 8 lateral triplane fractures and 3 medial triplane fractures. A tibial fracture was accompanied in 7 cases. On the anteroposterior radiographs, an oblique fracture extending superomedially from an inferolateral site and from an inferomedial site in the superolateral direction was observed in 4 and 3 cases, respectively. On the lateral radiographs, an oblique fracture extending from an anteroinferior site in a posterosuperior direction was observed in all 7 cases.
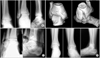
A closed and open reduction was performed in 6 and 8 cases, respectively. In 5 of the 7 cases with an accompanied femoral fracture, an open reduction was performed after an unsuccessful closed reduction. With regard to complications, degenerative arthritis was observed in 1 case (Fig. 2). According to the Modified Weber protocol, there were 13 excellent cases and 1 fair case, in whom traumatic arthritis had developed (Table 1).
DISCUSSION
Tillaux fractures and triplane fractures are the most common ankle joint fractures in adolescents with closure of the epiphyseal plate according to the mechanism of injury.6-8) The major mechanism of injury of triplane fractures are believed to be an external rotation force.1,9,10) According to the displaced fragment, lateral triplane fractures are caused by an external rotation force, whereas medial triplane fractures are believed to be the result of adduction. Dias and Giegerrich5) suggested that the external rotation force is the major mechanism of injury of triplane fractures, and postulated that a tibial fracture was accompanied during the application of a stronger external rotation force. In this study, a tibial fracture was found in 7 of the 14 cases, and an oblique fracture line could be observed on the anteroposterior and lateral radiographs. Therefore, it is believed that an external rotation force was the cause of the injury. Triplane fractures are characterized by radiographic evidence of the fracture lines in the sagittal, coronal and transverse planes, and their fracture pattern is not easy to identify. Nevertheless, precise identification of the fracture shape is essential for determining the treatment options and prognosis. A CT scan is commonly used to assess the extent of damage of a comminuted fracture and the articular surface as well as to locate the fragment site because plain radiography does not allow a precise evaluation. MRI is useful for diagnosing ligament injuries and osteochondral fractures.
Karrholm et al.11) reported that a CT scan as the most efficient method for assessing the shape of a triplane fracture, particularly two-part and three-part triplane fractures. Feldman et al.12) and Cone et al.13) reported that a CT scan was useful for determining the treatment method for triplane fractures and examining the status of the reduction and extent of displacement after surgery. In the present study, all patients underwent a CT scan, which was helpful in identifying the fracture shape that was barely distinguishable on the plain radiographs. In particular, the recently introduced 3-D CT scan has played an important role in assessing the fracture patterns and choosing the treatment options. Therefore, it is believed that more reasonable reduction methods can be provided with a proper understanding of the fracture shape and mechanism of injury.
In treating triplane fractures, attention should be paid to the fact that they are intraarticular fractures accompanied by growth plate injuries. In other words, complications, such as degenerative arthritis resulting from premature closure of the growth plate and articular surface incongruency can result in when proper treatment procedures are not followed. They require a precise anatomical reduction as with other intraarticular fractures. Accordingly, it is difficult to determine if a closed reduction alone can be enough or an open reduction should be performed. Marmor1) and Lynn14) pointed out the importance of surgical treatments. Meanwhile, Cooperman et al.4) reported that a closed reduction with cast immobilization resulted in satisfactory outcomes in 13 out of 15 triplane fracture cases but claimed that an open reduction was required in those combined with tibial fractures because the reduction could be disrupted due to the accompanied fractures. In the present study, satisfactory radiological results could be obtained with a closed reduction in 6 cases and accordingly, internal fixation and percutaneous K-wire fixation were performed. An open reduction was performed to achieve precise anatomic reduction when a closed reduction did not produce satisfactory outcomes, resulting in articular surface incongruency and ≥ 2 mm of displacement. In particular, 5 of the 7 cases with a combined tibial fracture underwent an open reduction. With regard to the traumatic arthritis observed in 1 case, it is believed that severe preoperative displacement and a failure to obtain a precise anatomical reduction during surgery led to the articular surface incongruency, which also resulted in arthritis. Therefore, considering that triplane fractures are growth plate injuries and intraarticular fractures, the decision for surgical treatment should be based on thorough preoperative plans using plain radiography and CT scans. Moreover, an open reduction is required when a precise anatomical reduction cannot be obtained with a closed reduction.
Arthroscopy is commonly used to diagnose and treat chronic ankle disorders with suspected intraarticular lesions and an osteochondral fracture of the talus, and is used to assess the level of reduction of intraarticular fractures, as described in recent reports. therefore, it is our understanding that arthroscopy can help reduce the risk of arthritis caused by intraarticular incongruency in cases of severe displacement and unsuccessful closed reduction.
It is believed that a CT scan is an efficient method for obtaining a precise assessment of the shape of triplane fractures. In addition, identifying the fracture pattern and understanding the mechanism of injury can result in an anatomical reduction and produce excellent clinical results.

 XML Download
XML Download