

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Osteonecrosis of the femoral head is a painful disorder that is found more commonly in middle aged men. Post-traumatic osteonecrosis of the femoral head has been found to result from vascular damage after trauma, such as a femoral neck fracture or hip dislocation. In contrast, the precise pathological mechanism of non-traumatic osteonecrosis is still unclear, and osteonecrosis can have a variety of causes, including alcohol abuse, steroid therapy, Caisson disease, Gaucher disease, radiation therapy, sickle cell anemia and atherosclerosis.
Regardless of the causes, most patients with osteonecrosis of the femoral head show similar clinical, radiographical and pathological findings, suggesting a common pathogenic pathway or causative factor. Some reports have suggested that the final step in osteonecrosis is vascular insufficiency to the femoral head,1) resulting in apoptosis (also known as programmed cell death) and necrosis. In addition, several recent studies reported that apoptosis is related to the pathogenesis of osteonecrosis of the femoral head.2,3)
An early diagnosis of osteonecrosis of the femoral head is difficult and most cases are diagnosed in an advanced and irreversible stage. Therefore, if the pathogenic mechanism of osteonecrosis involves apoptosis, the administration of apoptosis inhibitors, targeting the anti-apoptotic proteins, such as Bcl-2 and Bcl-xL,4) during the early stages of the disease might be effective in halting the disease progression.
Therefore, this study evaluated the expression of apoptosis in sections of femoral heads obtained during a total hip arthroplasty of patients with osteonecrosis, and the differences were analyzed according to the etiology.
METHODS
Materials
Of the patients diagnosed preoperatively with osteonecrosis and underwent total hip replacement arthroplasty between August 2004 and July 2005, 58 patients (58 hips) were available for this study. Their diagnoses were confirmed by the postoperative pathologic findings of osteonecrosis of the femoral head. Forty-one patients were males and 17 were females. The mean age of these patients was 53.7 years (range, 25 to 85 years) and the mean time from symptom onset to a definitive diagnosis was 2.1 years. According to a simple radiograph, 7 cases were Ficat stage II, 33 were III and 18 were IV. The causes of osteonecrosis were classified as steroid-induced, alcohol-induced, post-traumatic and idiopathic. Osteonecrosis was steroid-induced in 8 cases (13.8%), alcohol-induced in 29 cases (50%), post-traumatic in 6 cases (10.3%) and idiopathic in 15 cases (25.9%) (Table 1).
Staining Methods
Slides were made using stored femoral head sections fixed in 4% buffered formalin and embedded in paraffin. As a predealing process, the slides were incubated with 20 µg/mL proteinase K for 15 minutes, rinsed with phosphate buffered saline (PBS), incubated with 3µ H2O2 and methanol to block the endogenous peroxidase activity, and rinsed with PBS. The slides were terminal deoxynucleotidyl transferase mediated dUTP nick-end labeling (TUNEL) stained using an in situ cell death detection POD kit (Roche, Penzberg, Germany) in accordance with the manufacturer's instructions. All slides were counterstained with hematoxylin. As a negative control, the terminal transferase was omitted.
Immunofluorescence staining of a part of the slides was performed using the immunofluorescence marker included in the kit. The TUNEL-positive cells were found before diaminobenzidine (DAB) coupling because it is important to know that the slides made from stored specimens could be stained by the TUNEL method. After this pilot evaluation, all the slides were stained by DAB coupling.
Reading
Each slide was examined in 5 fields using the 400 high power field (HPF) of the microscope and the number of total and TUNEL-positive osteocytes in the trabecules of the non-necrotic portion around each necrotic lesion was counted. All slides were read by one musculoskeletal pathologist who was blinded to the evaluation and scoring. After calculating the average ratio of the number of TUNEL-positive cells to the total number of cells, the results were analyzed according to cause of osteonecrosis, and the significance of the statistical differences were evaluated using a Kruskal-Wallis test and Mann-Whitney U-test. The SPSS ver. 11.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis.
RESULTS
Of the patients with steroid-induced osteonecrosis, 5 were males and 3 were females. Their mean age at surgery was 44.3 years. Four cases had received kidney transplants and the other 4 cases received high-dose steroid therapies after neurosurgical operations. For patients with steroid-induced osteonecrosis, information on the exact total cumulative dose, mean daily dose, type of steroids, and duration of steroid therapy was unavailable.
Of the patients with alcohol-induced osteonecrosis, 28 were males and 1 was female. Their mean age at surgery was 54.7 years. All patients had a history of alcohol intake of more than 5 times per week. The average amount and period of alcohol intake was approximately 99.0 g per day and 25.7 years, respectively.
Of the patients with post-traumatic cases, 3 were males and 3 were females. Their mean age at surgery was 50.3 years. Five cases underwent total hip arthroplasty due to femoral neck fractures and the remaining case was treated with 2 months of traction for a traumatic hip dislocation.
Of the patients with idiopathic osteonecrosis, 5 were males and 10 were females. Their mean age at surgery was 57.8 years. In this group, the possible risk factors for osteonecrosis could not be found.
Using TUNEL immunofluorescence staining, no or few TUNEL-positive osteocytes were observed in the tissue samples of patients with post-traumatic or idiopathic osteonecrosis, whereas many positive osteocytes were observed in patients with steroid- or alcohol-induced osteonecrosis (Fig. 1).
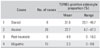
DAB coupling showed that the ratio of TUNEL-positive osteocytes was high in patients with steroid- and alcohol-induced osteonecrosis and low or rare in patients with post-traumatic and idiopathic osteonecrosis (Fig. 2). The mean percentages were similar in the steroid- and alcohol-induced groups, and in the post-traumatic and idiopathic groups (p > 0.05). However, there were significant differences between the former and latter two groups (p < 0.05) (Table 2). There were no significant differences in the number of apoptotic osteocytes according to the disease stages (p > 0.05).
DISCUSSION
The mechanisms of apoptosis and cell necrosis in ischemic conditions are radically different.1,5-8) Cell necrosis is always accompanied by the surrounding inflammatory reactions, whereas apoptosis occurs without inflammation. Apoptosis exerts a homeostatic function in relation to the tissue dynamics because the steady state of continuously renewing tissues is achieved by a balance between cell replication and cell death.9)
Several techniques have been used to detect apoptosis. The TUNEL method used in this study is based on the specific binding of the terminal deoxynucleotidyl transferase (TdT) to 3-OH (3-hydroxyl) ends of fragmented DNA from apoptotic cells, yielding polydeoxylnucleotide polymers.10) The TUNEL method makes it possible for direct observations and quantification of the fraction of cells undergoing apoptosis without damaging the tissue architecture. In some cells undergoing apoptotic cell death, DNA cleavage can be absent or incomplete. Moreover, steric hindrance, which can be caused by extracellular matrix components, can prevent the access of TdT to DNA strand breaks. In either case, false negative results can be obtained. Extensive DNA fragmentation can occur during the later stages of necrosis, which can result in false positive findings.11,12) Therefore, caution must be taken when interpreting the TUNEL results. Within each group, there was a wide range of TUNEL-positive cells, indicating the possibility of false positive and false negative errors in this study.
In this study, paraffin blocks were prepared routinely for a post-surgical histological examination. Although formalin cross-links proteins or peptides, thereby maintaining the morphological structure, long-term storage might reduce the antigenicity. Vis et al.13) reported that prostate needle biopsy specimens fixed in formalin, embedded in paraffin and mounted on glass slides showed a significant decrease in antigenicity after 5 years storage. However, the antigenicity was maintained when the tissue was archived in paraffin blocks and sectioned immediately before staining. Manne et al.14) reported similar results in breast tissues. Although these specimens had been stored for 3 to 15 months, it is likely that the antigenicity had been preserved because the glass slides were made from paraffin blocks immediately before staining.
The relationship between high dose steroid therapy and the development of osteonecrosis of the femoral head was first described in patients who underwent renal transplantation. Harrington et al.15) reported that approximately 34% of patients who ingested an average of 2,900 mg prednisolone during the first 3 weeks after transplantation developed osteonecrosis, compared to 10% of patients, who ingested an average of 1,200 mg prednisolone. In patients with systemic lupus erythematosus, a high initial corticosteroid dosage was suggested to be associated with the development of osteonecrosis.16,17) However, others reported that the total cumulative steroid dose and duration of steroid therapy were not related to the development of osteonecrosis, hence the causal relationship is unclear.18-20)
The pathogenesis of alcohol-induced osteonecrosis has not been defined but the pathological changes occurring in patients with steroid- and alcohol-induced osteonecrosis are similar.21) It was hypothesized that steroid- and alcohol-induced osteonecrosis of the femoral head are due to intraosseous hypertension caused by fat-cell hypertrophy and proliferation, fat embolism and a disturbance of the circulation.15) However, there is no definitive histological evidence of fat emboli during human osteonecrosis.22) Based on these findings, Glimcher and Kenzora23) suggested that steroids, alcohol and/or their metabolites affect osteocytes directly and cause apoptosis. They also proposed that the toxic metabolites may accumulate and induce apoptosis, particularly in areas in which venous stasis occurs, such as a femoral head.
It was proposed that apoptosis may be related to the pathogenesis of osteonecrosis of the femoral head.3) Calder et al.2) suggested that previously mentioned toxic metabolites might activate apoptosis modulators, such as inducible nitric oxide synthase (iNOS), leading to locally toxic levels of NO in osteoblasts and osteocytes followed by cell death or apoptosis and the development of osteonecrosis of the femoral head. Weinstein et al.24) reported that mice receiving glucocorticoids for 4 weeks exhibited a 3-fold increase in osteoblast apoptosis in vertebral cancellous bone, and osteoblast and osteocyte apoptosis was higher in patients with glucocorticoid-induced osteoporosis.
The percentage of TUNEL-positive osteocytes was high in the groups of patients with steroid- and alcohol-induced osteonecrosis, but was low or rare in patients with post-traumatic and idiopathic necrosis. These findings support the hypothesis that apoptosis plays a key role in the pathogenesis of steroid- and alcohol-induced osteonecrosis of the femoral head.
To date, studies of the relationship between apoptosis and osteonecrosis of the femoral head have been limited to a small number of patients or to animal models. Large case-control studies have not been performed and the precise pathogenic mechanism by which apoptosis causes osteonecrosis has not been defined. These findings suggest a need for further research into the role of apoptosis in the development of osteonecrosis of the femoral head.

 XML Download
XML Download