

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Lateral skin numbness is well known to orthopedic surgeons due to an infrapatellar branch of saphenous nerve (IPBSN) injury, which commonly occurs after knee joint surgery, but it is often underestimated and regarded as a trivial complication. Although it is unclear if damage to this sensory branch is clinically important, it can cause significant concern and problem in a few cases.1,2) This paper reports the results of preserving the infrapatellar branch of the saphenous nerve during unicompartmental knee arthroplasty (UKA) to prevent lateral skin numbness.
METHODS
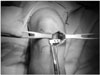
The targets of this study were 100 consecutive cases of UKA performed between September, 2004 and June, 2006 by a single orthopedic surgeon. All 100 cases had medial compartmental osteoarthritis and a minimally invasive technique had been used for UKA. Six cases were bilateral. There were 92 females and 8 males whose mean age, height and weight was 66.9 years (range, 57 to 82 years), 156 cm (range, 138 to 165 cm) and 62.3 kg (range, 43 to 81 kg), respectively. All patients underwent with Oxford Unicompartmental Knee Phase 3 (Biomet, South Wales, UK) under spinal anesthesia with a tourniquet on the proximal thigh. A slight longitudinal incision, starting from 1cm of the medial mid-portion of the patellar was made along the medial margin of the patellar tendon according to the tibial tuberosity. A careful dissection of the subcutaneous fat was performed to determine if the IPBSN lies above the fascia (Fig. 1). A colored rubber band was hooked to this nerve to prevent possible injury during surgery (Fig. 2). The joint space was opened up without dislocating the patellar and the set plan of the UKA was carried out (Figs. 3, 4, 5). In all cases, bone cement was used to fix the tibial and femoral component and a polyethylene bearing was inserted (Fig. 6). Careful closure was required to prevent injury to the IPBSN (Fig. 7). After closing the wound, an elastic bandage was used to compress the knee and leg. Partial weight bearing was encouraged using a walker on the first day after surgery. The sensory changes were evaluated 2 weeks after the procedure and repeated at 3, 6 months, and 1 and 2 years if any numbness was observed on the initial evaluation. The average follow-up period was 2 years and 8 months (range, 2 years to 3 years and 6 months). The results were recorded in terms of the classification of the IPBSN by Mochida and Kikuchi3) (Fig. 8), preservation after surgery, sensory changes to the lateral skin flap and complications. The extent of numbness was measured using a blunt pin for a pin-prick sensation and if any sensory loss was noticed, the dimensions were marked on a standard diagram of the knee with the incisions included.
RESULTS
The mean incision length was 6.7 cm (range, 5.5 to 8 cm) using a minimally invasive technique. The classification according to the location of IPBSN was observed as either Mochida Type I in 76 cases (76%), Type II in 16 cases (16%), and unclassified in 8 cases (8%) because the nerve appeared in multiple branches. In Type I, the IPBSN was saved in 62 cases (82%), and the mean distance from the joint line to the nerve was 9.13 mm (range, 4 to 15 mm), which was located inferiorly. However, in cases of Type II, the nerve was not preserved due to the surgical procedure. Thirty-eight cases had some degree of lateral skin numbness (Fig. 9). The mean area of numbness was 21.3 cm2 (range, 9 to 36 cm2). Among the patients whose IPBSN was preserved intraoperatively, 19 cases (31%) showed paresthesia or hypoesthesia that returned to normal 3 to 6 months after the operation. The rate of preservation of the nerve was 82% in Type I (62 cases out of 76). As a complication, one case had a neuroma that formed at the incision site but its symptoms were later relieved with a local steroid and lidocaine injection.
DISCUSSION
Lateral skin numbness can occur when an anteromedial incision is used in knee joint surgery. Although the IPBSN is well known to orthopedic surgeons, the numbness from the injury to this nerve is often dealt with as a trivial complication and overlooked. Anterolateral skin numbness of the knee is quite common after total knee arthroplasty due to an injury of this nerve. Borley et al.1) reported that two (7%) out of 25 total knee arthroplasty cases complained of critical discomfort in daily life. Although this had a low frequency, it can be a huge handicap according to the patients. Borley recommended that patients be informed of such complications and settle on an agreement prior to surgery. Of 113 total knee arthroplasty cases reported by Hopton et al.,4) 60% had subjective numbness, 20% were concerned that something had gone wrong with the knee replacement and 4.5% had significant problems with hypersensitivity that interfered with their activities of daily living. Hunter et al.5) suggested that complications due to an injury to the IPBSN could be prevented by making horizontal incisions in the medial compartment instead of longitudinal incisions. Berg and Mjoberg6) recommended the use of a lateral incision rather than a medial incision for cruciate ligament surgery of the knee joint. The anatomy of the saphenous nerve arises from the posterior division of the femoral nerve in the proximal thigh. It then enters the adductor canal in the adductor magnus, exits from the canal and divides immediately into its infrapatella and sartorial branches. The infrapatella branch pierces the sartorius muscle and then takes an oblique subcutaneous course to the medial border of the patella. The sartorial branch becomes subcutaneous by exiting between the sartorius and gracilis tendons, and passes distally to innervate the medial sensory of the leg and ankle.5,7) In Arthornthurasook and Gaew-Im's study8) of 37 cadavers, the IPBSN was classified according to its location in relation to the Sartorius, such as whether it was anterior, posterior, parallel, or through it. The most common type was the posterior type in 62% of subjects, in which the IPBSN penetrated the posterior margin of the sartorius and then distributed to the skin. In Ebraheim and Mekhail's study9) of 28 cadavers on the medial edge near the patellar tendon, the nerve passes by a set route, which can then be divided into a safe zone and a risk zone. Before a joint capsule incision or tibial intramedullary nail fixation, this nerve must be checked first and precautions must be taken to prevent injury. In Mochida and Kikuchi's study3) of 129 cadavers, the nerve passed by the medial joint line as Type I in 88 cases (68%), and did not as Type II in 41 cases (32%). The present study showed that 76 cases were Type I (76%), 16 cases were Type II (16%), and 8 cases (8%) were unclassifiable because the nerve branches had an atypical pattern. The symptoms that occurred after injury to this nerve were hypoesthesia, loss of sensation, parasthesia, neuroma, and reflex sympathetic dystrophy. Berg and Mjoberg6) reported that hypoesthesia decreases gradually with time. However, reinnervation did not work well in cases where the nerve was completely cut. Poehling et al.10) recommended preserving this nerve where possible because an unexplained persistent pain syndrome of the knee occurs as a result of reflex sympathetic dystrophy, which can cause significant concern to both the patient and doctor. These results showed that 76% of the nerve that was classified as Mochida Type I, had an average distance of 9.13 mm (range, 4 to 15 mm) from the medial joint line and passed inferiorly. This means that the location of this nerve can be predicted ahead of the procedure, which will help preserve it during the procedure. Therefore, if the nerve is not found above the joint line, the dissection must be made carefully because there is higher likelihood of the nerve being Type I, which was proven to be easily preserved in this study.
Many complications have been reported after total knee arthroplasty but important dissertations about this problem are still limited.1,2) On the other hand, many patients complain of the symptoms caused by the injury to this nerve after artificial knee arthroplasty. Many aspects of the patient's complaints were the possibility of a faulty operation, feelings of numbness, absurd sensations, tingling sensations, shocks and pokes, which placed the patients in a negative disposition. Hopton et al.4) reported that during total knee arthroplasty incision lengths greater than 22 cm had a regional area of skin numbness of 82.0 cm2. In contrast, the regional area of skin numbness was 31.7 cm2 when the incision length was less than 18 cm. Following Hopton's report, the length of the incision should be made as short as possible because increased length of the incision leads to increased chances of nerve injury as medial or intermediate cutaneous branches of the femoral nerve passes through the distal thigh.
The authors discovered that in cases of medial UKA, the preservation of this nerve was not difficult because the course of IPBSN is relatively constant, which is highlighted by the complete preservation rate in 82% of the Type I cases (62 cases out of 76) with a careful incision.
In conclusion, lateral skin numbness is highly expected with a possible division of the infrapatella branch of the saphenous nerve, even with a small skin incision in minimally invasive UKA. Attempts should be made to protect this nerve, even though it is questionable if it should be preserved during surgery. However, authors believe that it is worth trying to preserve this nerve.








 XML Download
XML Download