

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Pes planovalgus is the most common foot deformity observed in cerebral palsy (CP) patients. It is characterized by a loss of the medial longitudinal arch and malalignment of the foot, consisting of plantar flexion and valgus of the hindfoot, and abduction and supination of the forefoot. It becomes a clinical problem when pain or brace intolerance occur secondary to pressure medially over the prominent talar head. The treatment of this deformity should correct the foot malalignment, secure the stability of the foot during stance, and correct the abnormal gait by improving ankle plantarflexion at push-off and foot clearance during swing.
Classical Grice subtalar fusion1) may be complicated in children with neuromuscular diseases. Technical problems can often occur including instability or dislodgment of the cortical graft, undercorrection of hindfoot valgus, and overcorrection into varus.2-4) Metallic internal fixation for structural support was first reported by Dennyson and Fulford5) to decrease the pseudarthrosis and recurrence of the deformity. They also advocated the use of a cancellous bone graft instead of cortical bone struts to enhance bony fusion. However, previous studies only examined the clinical and radiographical outcomes.6,7) Furthermore, there are few reports on the results of extraarticular subtalar fusion performed exclusively in CP.2,4,6)
We reviewed our results of a modified Dennyson and Fulford technique using a cannulated screw and cancellous bone graft in CP patients with severe valgus feet. Three-dimensional kinematic and kinetic analysis of the ankle and dynamic foot pressure measurements were used to better understand the changes resulting from subtalar stabilization.
METHODS
The study design was a retrospective review and was approved by our hospital's institutional review board. Between 2000 and 2004 at our institution, 48 consecutive patients underwent extraarticular arthrodesis of the subtalar joint for a planovalgus foot deformity that was painful and resistant to orthotic management. The patients were included in the study when they met the following criteria: 1) could walk independently without any assistance prior to surgery, 2) had no previous foot surgery, 3) had no concomitant surgery for forefoot or midfoot during the index operation, and 4) had a minimal follow-up of 2 years after surgery.
The study population consisted of 50 feet in 30 patients (21 boys). The mean age at the time of surgery was 9 years (range, 5 to 18 years), and the mean follow-up period was 37 months (range, 26 to 49 months). Eight patients underwent a selective dorsal rhizotomy before the index operation and all patients had had a crouch gait, which was defined according to the sagittal plane kinematics as ankle dorsiflexion of > 15° and knee flexion of > 30° during the late stance phase of the gait.8)
In all patients, the index operation was performed as one of multi-level and simultaneous procedures of the lower extremities designed to improve the entire gait pattern.9)
Twenty patients underwent the index operation bilaterally. Ten patients underwent the index operation, unilaterally and calcaneus-cuboid-cuneiform osteotomy described by Rathjen and Mubarak,10) on the other foot and choice of the procedure was made according to the surgeon's preference. Psoas recession over the pelvic brim were performed in 19 patients, adductor tenotomies in 18, distal medial hamstring lengthenings in 27, rectus femoris transfer to sartorius in 8, and patellar tendon advancement with supracondylar extension osteotomy of the femur in 6. To obtain normal rotational profiles of the femur and/or the tibia, supramalleolar derotation osteotomy of the tibia was performed in 13 patients, and an inter- or subtrochanteric derotation osteotomy of the femur was performed in 11. No patient underwent a supramalleolar osteotomy because of a valgus deformity at the distal tibia.
Surgical Techniques
Extraarticular subtalar arthrodesis with a modified Dennyson-Fulford technique was performed by a single surgeon (HWK). Briefly, an obliquely placed incision that follows the normal skin lines was made along the anterolateral aspect of the foot on the sinus tarsi. The origin of the extensor digitorum brevis was taken down and reflected distally in a tongue-like manner, and the sinus tarsi was cleaned of all fat and soft tissue. The dorsum of the talar neck was also exposed through the interval between the extensor digitorum longus and anterior tibial neurovascular bundles.
The calcaneus was rotated under the talus, and the hindfoot was held in the corrected neutral position with the ankle in equinus. The reduction status of the talonavicular joint was confirmed under the intraoperative fluoroscopic control, and a satisfactory position was defined as when the long axes of the talus and navicular aligned valgus approximately 5° in the anteroposterior projection. A threaded guide wire was driven from the talar neck into the calcaneus in the posterolateral direction to emerge through its lateral cortex near the plantar surface. After drilling but not tapping the bone, an appropriate-sized AO cannulated screw (3.5 mm, 4.5 mm, or 7. 0 mm diameter, depending on the size of the bone) was inserted to hold the foot while the graft was incorporated. The undersurface of the talus and the upper surface of the nonarticular calcaneus were decorticated using a dental bur, and the sinus tarsi was then packed with an iliac cancellous bone graft. Intramuscular lengthening or Z-plasty of the tight peroneus brevis tendon was performed in 42 feet. Eight gastrocnemius resections and 38 tendo-Achilles lengthenings were performed for the correction of equinus deformity. Four patients had undergone tendo-Achilles lengthenings at other institutions before the index operation.
Postoperatively, all feet were immobilized in a long leg cast for 4 weeks, and then in a short leg walking cast for another 4 weeks. For most patients, a posterior leaf-spring or hinged ankle-foot orthosis was prescribed after removing the cast. The screw was not removed routinely, and was left in situ if the patients were asymptomatic.
Outcome Measures
Standardized standing anteroposterior and lateral radiographs of the feet and ankles of each patient were taken before surgery and at the latest follow-up. The talo-1st metatarsal angle and talocalcaneal angle were measured on the AP view, and the lateral talocalcaneal angle, calcaneal pitch angle, Meary angle (lateral talo-1st metatarsal angle), and Hibbs' angle (lateral calcaneus-1st metatarsal angle) were measured on the lateral view.11) Additional information from the radiographs included the time to fusion, presence of pseudarthrosis and metal failure.
Kinematic and kinetic analyses were performed using the VICON 370 Motion Analysis System (Oxford Metrics, Oxford, UK) with 6 infrared cameras, and information on the ground reaction force was gathered using multiple force platforms (Advanced Mechanical Technology, Watertown, MA, USA). All subjects were asked to walk barefoot at a self-selected speed along a 15 meter walkway with the markers in place. The normal range for kinematics was defined as two standard deviations around the average. Force-plates under the path recorded ground reaction forces during the walking trials, and joint moments were expressed as the internal moments to counter the ground reaction force.
Kinematic and kinetic data from successful trials were averaged and used for statistical analysis.
The Tekscan High Resolution Pressure Assessment System (South Boston, MA, USA) was used to measure the dynamic foot pressure. The system consists of a 61 × 65 cm2 pressure-sensitive floor mat containing a grid of 87 rows and 96 columns of pressure-sensing cells, and the pressure was recorded at 60 Hz. Foot pressure in 9 areas, including the hallux, 1st metatarsal head (1st MT), 2nd metatarsal head (2nd MT), 3-4th metatarsal heads (3-4th MT), 5th metatarsal head (5th MT), medial midfoot (Med M), lateral midfoot (Lat M), medial calcaneus (Med C), and lateral calcaneus (Lat C), were recorded for 5 steps in the middle of the test walk and the mean value was calculated (Fig. 1).
The pressure-time data for each individual area was graphed using a normalized pressure and time scale. The integrals of the pressure-time graphs indicate the total pressure achieved by each area of the foot, which was identified as the "impulse" for this study. The relative vertical impulse (RVI), which is the percentage of the impulse exerted on each area out of the total impulses of all areas, was the key foot (plantar) pressure parameter examined in this study.12,13) Therefore, the data was unaffected by body weight, plantar surface area, size of the foot, or contact time of the foot during walking (Fig. 2). The other parameters examined included the anteroposterior index (API) and the center of the pressure excursion index (CPEI), which are used to evaluate the anteroposterior and lateral movements of the center of pressure, respectively.13,14) The presence or absence of medial deviation of the path of the center of pressure immediately after heel strike was observed to assess the absorption of the impact caused by the pronation movement occurring in the subtalar joint (Fig. 3).13,15)
Statistics
Statistical analysis was performed using the SAS ver. 9.1 (SAS Ins., Cary, NC, USA) and the level of significance was set at p < 0.05. To determine the effect of surgery and to allow for repeated measurements of individual patients, the mixed model was used to compare the measured values of the plain radiographs and dynamic foot pressure measurements taken before surgery and at the latest follow-up. In addition, the plantar pressure data obtained in the patients were compared with the normative database of age-matched 30 healthy volunteers, aged 6 to 20 years. A mixed model was also used to compare with the normal control group.
RESULTS
At the latest follow-up, there was no recurrence of the planovalgus foot deformity in any of the patients. None of the patients developed other types of foot deformity, and all arthrodeses healed radiographically after 9 weeks (range, 6 to 11 weeks). There were no screw fractures or infections. Complications included 3 heel sores and 2 cases of marginal necrosis of the incision wound, which was resolved quickly with local wound care. All patients except for the above 2 reported no foot pain at walking after surgery. The other 2 patients reported subcutaneous irritation and pain due to proximal migration of a screw but no pseudarthrosis. The pain disappeared after removing the screws. Although we did not perform full gait study postoperatively for all patients, all patients showed a more upright posture and increased knee extension during stance after surgery.
On the anteroposterior radiographs, the talo-1st metatarsal angle and talocalcaneal angle decreased postoperatively. On the lateral radiographs, the Meary angle and Hibbs' angle were lower at the latest follow-up. The lateral talocalcaneal angle was decreased after surgery, and the calcaneal pitch angle was increased slightly postoperatively but it had not improved significantly after surgery (Fig. 4 and Table 1).
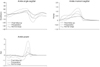
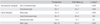
Peak dorsiflexion of the ankle during stance phase was increased after surgery, and the peak plantarflexion at push off was decreased (p < 0.05). The peak ankle plantar flexion moment and power were also decreased (p < 0.05) (Fig. 5 and Table 2).
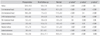
Prior to surgery, the RVI of the hallux and 1st MT were higher than those of the normal control. The RVI of the 2nd MT was similar to the normal control. The RVI of the 3-4th MT, 5th MT, lateral midfoot, and calcaneus were lower than the normal control. However, the RVI of the medial midfoot was higher than that of the control group. The RVI of the hallux decreased after surgery and recovered to the normal level. The postoperative RVI of the 1st MT and 2nd MT were decreased to a lower level than that of the normal control. The RVI of the 3-4th MT and 5th MT was not changed after surgery. The postoperative RVI of the lateral midfoot had increased while that of the medial midfoot decreased but both were higher than normal. The RVI of both the medial and lateral calcaneus increased to a level higher than normal (Fig. 6 and Table 3).
The API increased from 49 ± 14% preoperatively to 64 ± 8% postoperatively (p < 0.01) but the postoperative API was lower than normal (79 ± 2%, p = 0.04). The CPEI was increased from 16 ± 9% before surgery to 21 ± 6% after surgery (p < 0.01), and the postoperative CPEI was similar to that of the normal control (20 ± 5%, p = 0.07). Preoperatively, medial deviation of the path of the center of pressure was observed in only 4 feet. In contrast, more distinct medial deviation of the path of the center of pressure was observed in 25 feet after surgery.
DISCUSSION
Surgical treatment for pes planovalgus that is resistant to orthotic management includes subtalar arthrodesis, medial sliding calcaneal osteotomy10) and lengthening osteotomy of the os calcis.16) The long-term results of the latter two procedures remain unsettled. Nevertheless, calcaneal osteotomies are usually recommended for a mild to moderate degree of the deformity and they have the added bonus of maintaining joint motion. On the other hand, extraarticular arthrodesis of the subtalar joint is recommended as a means of correcting severe hindfoot valgus.
The radiographic findings of a reduction of the talo-1st metatarsal angle after surgery reflect the correction of abduction of the forefoot and subluxation of the talonavicular joint. The reduction of the anteroposterior talocalcaneal angle suggests an improvement in the hindfoot valgus. A decrease in the Meary angle and Hibbs' angle suggest an improvement in the malalignment of the talonavicular joint and medial longitudinal arch, respectively. Hadley et al.7) reported that flexion of the talus was corrected after surgery, and this was represented as a reduced lateral talocalcaneal angle. In this study, the lateral talocalcaneal angle decreased, probably because the plantar flexion of the talus had been corrected but the calcaneal pitch was not improved with the index operation. Since both the talus and calcaneus are in equinus in a spastic valgus deformity of the hindfoot, the lateral talocalcaneal angle can be considered to have been decreased even to a level lower than normal if the equinus of the calcaneus is not corrected properly. It is believed that simply holding the heel in a neutral position and the ankle in equinus, as a step to correct planovalgus during the index operation, cannot correct the equinus of the calcaneus as well. The AP talo-1st metatarsal angle was measured in the operating field but this would simply be a uniplanar observation of a restoration of the alignment of the talonavicular joint.
Although the changes in dynamic foot pressure were analyzed to examine the effects of the index operation, simultaneous additional multilevel-surgery may have had an influence on the presented foot pressure results. However, the dynamic plantar pressure measurements can allow assessments of the patients' overall ability to support and efficiently transfer the body mass during ambulation.15,17,18) In particularly, relative vertical impulse is independent of the spatiotemporal and anthropometric parameters.13,15) Due to the wide variation in the shape and size of the feet, it may not be reasonable to average the foot pressure data in a manner comparable to the radiographic measurements. The plantar pressure was examined by subdividing the foot into 9 areas, and the relative vertical impulse was calculated to allow comparisons between individuals of different sizes and ages. The RVIs of the hallux, 1st metatarsal head, and medial midfoot were decreased, while that of the lateral midfoot was increased after the index operation. The increased RVI of the lateral midfoot and the decreased RVI of the medial midfoot represent a postoperative elevation of the medial longitudinal arch. However, a higher than normal RVI of the medial midfoot suggests that the medial longitudinal arch had not been restored completely.
Ledoux and Hillstrom14) determined the distributed plantar vertical force in the neutrally aligned normal feet and flexible flatfoot, and observed that the flatfeet had more force at the subhallucal area. They attributed this to the inappropriate exertion of the peroneus longus due to malalignment of the foot and abnormal activation of the flexor hallucis as compensation.19) Furthermore, this might be indicative of aberrant first ray mechanics in flatfeet. Postoperative normalization of the RVI of the hallux in this series suggests a disappearance of abnormal activation of the flexor hallucis after surgery. In addition, the higher than normal RVI of the 1st metatarsal head before surgery and the lower than normal RVI after surgery can be interpreted as a consequence of uncorrected forefoot supination and incompetent function of the peroneus longus.20) This is not a consequence of an overcorrection of the talonavicular joint because postoperative RVI of the medial calcaneus was still higher than that of the lateral calcaneus. Although there is no single procedure that can correct three-dimensional planovalgus foot deformity, it is believed that the index operation reliably corrects the hindfoot valgus deformity in patients with spastic diplegia.
The center of pressure is the mean pressure applied to the sole of the foot. During a normal gait, the path of the center of pressure is initiated from the center of calcaneus, deviates to the lateral side of the foot, and ends near the 2nd metatarsal head.13,14) If the foot pronates, the path of the center of pressure will tend to move medially, whereas it tends to move toward the lateral border upon supination. The finding of an increase in the center of the pressure-excursion index after surgery indicates a shift in the path of the center of pressure through the lateral midfoot after initial contact and an elevation of the medial longitudinal arch. An increase in the anteroposterior index of the path of the center of pressure and increase in the RVI of the calcaneus after surgery suggest an increased excursion of the gastrosoleus musculotendinous unit and correction of "lever-arm diseases" of the lower extremity as well as an elevation of the medial longitudinal arch. However, the higher than normal RVI of calcaneus, lower than normal RVI of the metatarsal heads, and the lower than normal anteroposterior index suggests that the patients in this series still have incompetent plantar flexion-knee extension couple even after multi-level corrective surgery. The medial deviation of the path of the center of pressure immediately after initial contact indicates shock absorption by the pronation of the subtalar joint.15) In the present study, such shock absorption at the subtalar joint was obvious in 50% of cases after surgery. However, it is possible that this finding was caused by compensatory movement at the ankle joint. These findings suggest that the peak dorsiflexion of the ankle was increased after surgery. The ankle plantarflexion-knee extension couple should be effective for sufficient ankle plantarflexion at push-off. Sufficient ankle dorsiflexion during mid-stance is the prerequisite of knee extension, and can be obtained by the lengthening of the shortened triceps surae musculotendinous unit. However, postoperative reduction of the ankle plantarflexion angle, moment, and power suggest that the patients in our series still have insufficient ankle plantarflexion-knee extension, even with a correction of the lever-arm disease of the foot and ankle.
Although Bourelle et al.21) reported no deformity of the talus or arthritis of the adjacent joints 17-22 years after Grice extraarticular subtalar arthrodesis, it is unclear if stiff fusion will eventually result in premature articular changes with ankylosis of the joints involved and reduced movement.






 XML Download
XML Download