

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Coblation devices are essential in arthroscopic procedures for rapid hemostasis, clearing the visual field, easing problematic procedures and shortening the operation time. The function of coblation devices is determined by the type of wands. The Super MultiVac 50 (Arthrocare Corp, Sunnyvale, CA, USA) is a suction wand and it is useful to enhance visibility during bloody arthroscopic surgeries. We report here on the case of a separated coblation wand tip (Super MultiVac 50) and we removed the tip from the popliteal hiatus of the knee. Moreover, we describe the cause of the instrument failure in our case.
CASE REPORT
A 55-year-old man injured his right knee in a traffic accident and he sustained bicondylar fractures of the proximal tibia, which were managed by open reduction and internal fixation. The postoperative course was uncomplicated, but his range of motion (ROM) for the knee was limited in spite of vigorous physical therapy. At 7 months after the surgery, he had ROM with a 15° lack of knee extension and a 100° lack of knee flexion. Arthroscopic release was planned for the treatment of the arthrofibrotic knee.
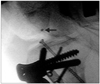
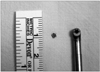
During the coblation of fibrotic tissue in the intercondylar notch, a tip of the Super MultiVac 50 wand separated and went out of sight. We continued to arthroscopically examine the knee, but could not see the tip of the wand. Using C-arm fluoroscopic control, we discovered the separated tip in the posterolateral compartment of the knee (Fig. 1). We tracked the wand tip with the arthroscope in the popliteal hiatus of the knee (Fig. 2). The separated wand tip was light and round-flat-shaped with a diameter of 3 mm (Fig. 3). To find the lost tip, the helpful procedures we employed were to stop the flow of irrigation fluid, use C-arm fluoroscopy and to minimize the joint motion. The separated tip was easily taken out and intra-articular adhesiolysis of the knee was done completely. Two months later, the patient had full range of knee motion.
DISCUSSION
In arthroscopic surgery, instrument failures, and mainly the breakage of instruments, are rare complications with low incidences. However, reports of various iatrogenic foreign bodies have increased with the diversified usage of this procedure. There are several reports of migration of interference screws after anterior cruciate ligament reconstruction.1,2) Various other materials that have been found as iatrogenic foreign bodies include broken basket forceps,3) broken blade tips4,5) and broken bone staples.6) In most cases, the broken fragments were noticed instantly, yet in some cases,3,7) the detached tips were undetected during arthroscopic surgeries. In the cases of a No. 11 blade4) and a broken blade5) that were missing within the knee joint, the surgeons had to make an incision to retrieve them from the joint. Early recognition of instrument failure may prevent any associated morbidities, such as a reoperation or subsequent cartilage damage. We present the case of a separated wand tip, and this case should make surgeons aware of the potential problems associated with the use of coblation wands.
The separated tip of a wand was round-flat-shaped with a diameter of 3 mm and as light as a feather. After it was missing in the suprapatellar pouch of the knee joint, it disappeared from our arthroscopic field of vision. The helpful procedures to find the lost tip were to stop the flow of irrigation fluid, use C-arm fluoroscopy and minimize the joint motion. We were able to remove the tip from the popliteal hiatus, which is where loose bodies of a knee joint could reside.
Some hypotheses can be speculated regarding the etiology of separation of the wand tip. As an economizing measure, we commonly used a reprocessed wand that is sterilized by Ethylene Oxide. We consulted the Arthrocare Corporation about the expected life span of Arthro Wands (Arthrocare Corp, Sunnyvale, CA, USA) and the effect of reprocessing. With regards to the "burn time" for a Super MultiVac 50, they recommend no more that 7 minutes (continuous or accumulative) on the set point 9 (maximum setting). Reprocessing of single-use Arthro Wands is not recommended because it may negatively affect the device's functional integrity. In our patient's case, we used a reprocessed Arthro Wand and we simply overworked it. Another possible cause of failure would include the wand going in and out the joint without an arthroscopy cannula. For the patients safety and to prevent such problems, we report here on what happened during this case to help others in the orthopedic community. Emphasis has be placed on routinely inspecting all instrumentation before and after entering the knee joint to eliminate any chance of inadvertently leaving behind any foreign body.

 XML Download
XML Download