

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Placement of endosseous implants has become a predictable option in comprehensive periodontal treatment planning for both fully and partially edentulous patients. The initial stability of an implant is a critical factor for the achievement of osseointegration1). But, it is often difficult to obtain proper implant stability in soft bone. The lack of initial stability in soft bone can lead to lower success rates, which can vary from 50% to 94%2). Occasionally, the placement of implant in the posterior maxilla is limited by insufficient bone volume. However, it can be solved by sinus augmentation using various surgical procedures3-5). Indeed, when the width and height of residual alveolar ridges were significantly modified after tooth extraction, it may jeopardize the correct implant placement and stability. To effect more ideal implant placement or allow the fabrication of better restorations, the application of the principle of guided bone regeneration (GBR) has become a predictable treatment option in implant dentistry6-7).
Since the 1980s, it has been tried to overcome the high failure rate of machined surface implants and gain adequate primary stability in sites with poor bone quality and quantity. Firstly, the evolution of implant design has been proposed. Many manufactures developed more variable implants using an increase in implant diameter, double-spiraled thread or root shape anatomy. Secondly, bone condensation using osteotomes was proposed by Summers8). This is an useful and a predictable procedure for implant placement in soft maxillary bone. Finally, the development of new surface textures has been studied widely with the aim of improving the initial implant stability and bone healing. There are many implants of new surface, but we were interested in two typical implant surfaces. One is a novel titanium porous oxide implant surface (Ti-Unite™) which has been introduced by the Nobel Biocare AB (Gothenburg, Sweden) since 2000. The highly porous titanium oxide layer is thickened toward the apex of the threaded root-form oral implant. The other is a sandblasted large-grit acid etched implant surface (SLA) which has been proposed by the Straumann Institute since the early 1990s. The titanium surface is first sandblasted with large particles causing a grossly rough surface which is secondarily acid-etched, forming a finely rough surface.
Recently, a few studies have compared Brånemark System® implants with ITI System® implants. SLA ITI implants (98%) have a significant higher survival rate than machine-surfaced Brånemark implants (81%) in autogenous grafted maxillary bone9). In a 3-year follow-up of a randomized study, there was a high survival rate (97.3%) and low marginal bone loss for both ITI (TPS surface) implants and Brånemark (turned surface) implants in the treatment of a partially edentulous maxilla10). The simultaneous placement of the Brånemark Ti-Unite™ and ITI SLA implants with BAOSFE procedure showed a predictable clinical results during the observation periods of 12 months. The Brånemark Ti-Unite™ implants showed 100% survival rate and the ITI SLA implants showed 94.4% survival rate11). In the atrophic posterior maxilla with sinus floor elevation procedure, the survival rate was 96.4% in Brånemark Ti-Unite™ implants and 98.8% in ITI SLA implants12).
However, there have been few studies that have compared the survival rate between the Brånemark Ti-Unite™ implants and the ITI SLA implants in soft bone. The aim of this study was to compare the survival rate of Br™nemark Ti-Unite™ implants and ITI SLA implants in soft bone.
MATERIALS AND METHODS
1. Patients and Implants
In the Brånemark Ti-Unite™ (Nobel Biocare AB, Gothenburg, Sweden) group, 84 patients (39 men and 45 women, mean age of 54 years, age range of 21 to 75 years) were treated with 201 Brånemark Ti-Unite™ (BRA) MK III or MK IV implants between May 1999 and May 2004. In the ITI SLA (Straumann Institute, Basel, Switzerland) group, 74 patients (44 men and 30 women, mean age of 57 years, age range of 21 to 81 years) were treated with 120 ITI SLA (ITI) implants between December 2000 and May 2004. The patients were followed-up 0~5 years in ITI group or 0~6 years in BRA group, respectively. The patients were mainly healthy or had well-controlled systemic disease. All implants were placed in soft bone at the Department of Periodontology, College of Dentistry, Yonsei University.
2. Implant distribution
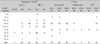
In both groups, the implants were mainly placed in the posterior maxilla (Table 1) or the type C bone (Table 2) in accordance to the Lekholm and Zarb index13). As shown in Table 3, MK IV implants were mostly installed in the BRA group (81.1%), and ITI solid screw implants were mostly installed in the ITI group (75.8%), respectively.
3. Study design
This study was carried out retrospectively using the patients' chart. The following information was collected from the patient records: age, gender, systemic disease, the type, number, length and diameter of the implants, their location in the jaws, bone quantity, the number of failed implants, the causes of failure, and advanced surgery for bone augmentation [Osteotome Sinus Floor Elevation (OSFE), Bone Added Osteotome Sinus Floor Elevation (BAOSFE), Sinus graft (1-stage), Sinus graft (2-stage), and GBR].
4. Survival criteria
The survival rates were calculated according to the method reported by Buser et al14) as follows:
5. Statistical analysis
The results were evaluated using the life table analysis described by Cutler & Ederer.15) The differences in the survival rates between the implant types were examined using a Mantel-Haenszel chi-square, and the differences among the advanced surgical techniques were examined using the Fisher's exact test.
Results
1. Cumulative survival rate
In the BRA group, 2 submerged implants were lost before healing abutment connection following flap dehiscence with suppuration, 5 submerged implants were lost at the time of abutment connection and 1 non-submerged implant was lost 5 weeks postoperatively following healing abutment loosening and fixture mobility. Of the failed implants, one upper anterior implant (MK IV Ø 4 × 15 mm, # 11 area) was installed 7 weeks after removal of MK II Ø 3.75 × 18 mm. The previous MK II implant was installed with GBR technique because of labial bone penetration, but it was lost 10 months postoperatively due to repeated pus discharge. One lower posterior implant (MK III Ø 3.75 × 13 mm, #45 area) was failed at the time of healing abutment connection. The six upper posterior failed implants (MK III Ø 5 × 8.5 mm, #26, 27 area MK IV Ø 4 × 13 mm, # 25 area; MK IV Ø 5 × 8.5 mm, # 16, 26 area; MK IV Ø 5 × 11.5 mm, # 25 area) were related to sinus augmentation. One MK III Ø 5 × 8.5 mm fixture on # 26 area was installed with sinus membrane perforation at the time of OSFE technique. Two patients (3 implants) had smoking habit and one patient (1 implant) had bruxism, and one patient (1 implant) had a stable angina pectoris. A total of 8 implants failed early, resulting in a 96.02% survival rate. After loading, one implant (MK IV Ø 4 × 13 mm, # 24 area) was lost at the 7th month after using an overdenture due to overloading, resulting in a cumulative survival rate of 95.48%. In the ITI group, no implant was removed but one implant (ITI TE™ Ø 4.1 / 4.8 × 12 mm, # 27 area) showed repeated suppuration after installation of the permanent prosthesis. After being treated with antibiotics, chlorhexidine irrigation, and curettage, the peri-implantitis was controlled. The implant was left in place but a suppurative peri-implant infection was found at the last annual examination. This implant was considered to be a failure, resulting in a cumulative survival rate of 99.10% (Table 4, Fig. 1). Therefore, there were 1of 120 failure in the ITI SLA implants and 9 of 201 failures in the Brånemark Ti-Unite™ implants, respectively. However, there was no significant difference between both groups (Mantel-Haenszel =0.138).
2. Survival rate for each surgical method
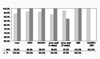
The surgical methods used at the time of implant placement are described below (Table 5). In the case of OSFE, or 1-stage sinus graft, or 2-stage sinus graft, respectively, there was higher percentage of BRA cases than ITI cases. Figure 2 shows the survival rate according to the additional surgical procedures and implant type. In all cases, the survival rate was not significantly different in the two implant types according to Fisher's exact test (p>0.05).
Discussion
Many studies have demonstrated that a lack of initial stability in soft bone, particularly in the posterior maxilla, leads to lower success rates than in other locations and bone qualities16-18). In order to overcome the high failure rate of implants in soft bone, a modification of the surgical methods during implant placement has been suggested that bone condensation with osteotomes, minimal or no countersinking, not to drill to the total implant length, and light forces during implant insertion. In addition, wide diameter implant, wide collar, and the implant design for increasing the surface of bone to implant contact are recommended. Finally, the implant surface texture have been modified to enhance the cellular activity and primary stability. Rough surfaces of implant are advocated not only to increase primary stability but mainly to improve bone healing2). To improve the initial implant stability, high removal torques and maximize the quality of the bone-implant interface, a novel titanium porous oxide implant surface or a sandblasted large-grit acid etched implant surface are studied respectively19-22). However, there have been few studies that have compared the survival rate between both implants in soft bone.
In this study, 201 (BRA) and 120 (ITI) implants were placed in soft bone. Among the 8 early failed implants (BRA), 6 implants were related to the sinus augmentation procedure in the posterior maxilla, and 2 implants were rotated at the time of healing abutment connection because of osseointegration failure. There was only 1 implant failure within 1 year after loading in each group, and no implant failed in both group after 1 year. Therefore, the cumulative survival rate was 95.48% in BRA group, and 99.10% in ITI group, respectively. At the time of implant placement, none or the BAOSFE method were more frequently used in the ITI group, while other procedures were more frequently used in the BRA group. The survival rates in the BRA group (97.5%) and ITI group (87.5%) were significantly different in the case of sinus graft (2-stage). However, there was no overall significant difference between the two groups because the number of implant placement in the ITI group (8) was significantly lower than in the BRA group (40). The cumulative survival rate and overall survival rate for each surgical method was similar in the two groups (Mantel-Haenszel=0.138 and Fisher's exact test>0.05, respectively), and this results were comparable to previous study23).
High survival and success rates (90.7-100%) for the two systems have been individually reported in many earlier studies24-37). Regarding the Brånemark Ti-Unite™ implant placement in type 4, Glauser et al24) demonstrated a 97.1% success rate after 4 years of prosthetic loading in soft bone. In addition, Friberg et al25) reported a 96.2% survival rate over a follow-up period of 1 year. Likewise, Pinholt9) r eported a 98% overall survival rate of ITI SLA surface implants in the human bone-grafted maxilla, bone quality 4, over a follow-up period of 20-67 months. Stricker et al26) demonstrated a 99.5% survival rate after 15-40 months of implant placement during maxillary sinus augmentation with autogenous bone grafts. Therefore, the survival rate in the BRA group (95.48%) and ITI group (99.10%) in this study is comparable to other studies. In this retrospective article, most cases had been applied a delayed loading after the placement of implant. Further studies will be needed to evaluate the radiographic changes over a long follow-up period in each implant system and to study the survival rate after immediate loading.
In conclusion, the survival rates of the oxidized titanium implants and the sandblasted large-grit acid etched implants were similarly high in soft bone. Both implants can be used successfully in soft bone regardless of the surgical methods used at the time of implant placement.





 XML Download
XML Download