

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
The non-carious cervical lesion(NCCL) is a loss of tooth structure at the neck of affected teeth that is unrelated to tooth caries. The reported prevalence of NCCL varies from 5% to 85%. Prevalence and severity of lesions have been found to increase with age. They are becoming more significant as people live longer and become more aware of the importance of oral health. The purposes of this study were first, to examine the periodontal conditions associated with NCCL, and second, to investigate the clinical effects of class V restorations of NCCL on periodontal tissues.
Materials and methods
The sample size was 982 teeth of 50 subjects(25 male, mean age 52±7) who were seen at the Department of Periodontology, Pusan National University Hospital. At the baseline examination, clinical periodontal parameters were measured. After the initial examination, 24 patients who were absent from hypersensitivity were selected. The teeth with NCCL were randomly divided into the test and control groups. The teeth in the test group were restored with flowable resin; the control teeth were not restored. Six months later, the clinical examinations were repeated. The data were analyzed using the SPSS program.
Results
The results were as follows: 1) NCCL occurred on 45.8% of examined teeth. The percentage of affected teeth was higher in maxillary and premolar teeth. 2) The shallow saucer type was the most common. 3) Teeth with NCCL had more gingival recession, lower attachment level, and higher incidences of bleeding on probing(BOP) and plaque than NCCL-free teeth. 4) Six months later, gingival recession, attachment level, the percentages of BOP and plaque in the test group were lower than in the control group(p<0.05).
Figures and Tables
 | Figure 1Angular shape of cervical lesion in buccolingual cross section. (A) Wedge shape, (B) Saucer shape
|

 | Figure 3The Distribution of the non-carious cervical lesions according to their location and shape. All the population had more than one non-carious cervical lesion.
|


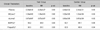
Table 3
Relationship Between the Clinical Parameters and Shape of the Non-Carious Cervical Lesions(NCCL)

![]()



Table 7
Comparison of the Clinical Parameters Between the Test Group and the Control Group
Test group: restorative treatment was done
Control group: restorative treatment was not done
PD: Probing depth; GR: Gingival recession; AL: Attachment level; BOP: Bleeding on probing
PD, GR, AL: Paired t-test was used to test statistically significant change between baseline and 6month later(p<0.05). mean±SD
Independent t-test was used to test statistically significant change between test and control group at 6month later(p<0.05). mean±SD
BOP, Plaque: Mcnemar test was used to test statistically significant change between baseline and 6month later, as well as test and control group at 6 month later(p<0.05).
*: Statistically significant difference between test and control group at 6month later(p<0.05).
![]()
References
1. Osborne-Smith KL, Burke FJ, Wilson NH. The aetiology of the non-carious cervical lesion. Int Dent J. 1999. 49:139–143.

2. Aw TC, Lepe X, Johnson GH, Mancl L. Characteristics of noncarious cervical lesions. A clinical investigation. J Am Dent Assoc. 2002. 133:725–733.
3. Levitch LC, Bader JD, Shugars DA, Heymann HO. Non-carious cervical lesions. J Dent. 1994. 22:195–207.
4. Sangnes G, Gjermo P. Prevalence of oral soft tissue and hard tissue lesions related to mechanical tooth cleansing procedures. Community Dent Oral Epidemiol. 1976. 4:77–83.
5. Hong FL, Nu ZY, Xie XM. Clinical classification and therapeutic design of dental cervical abrasion. Gerodontics. 1988. 4:101–103.
6. Donachie MA, Walls AW. Assessment of tooth wear in an ageing population. J Dent. 1995. 23:157–164.
7. Borcic J, Anic I, Urek MM, Ferreri S. The prevalence of non-carious cervical lesion in permanent dentition. J Oral Rehabil. 2004. 31:117–123.
8. Bader JD, McClure F, Scurria MS, Shugars DA, Heymann HO. Case-control study of non carious cervical lesions. Community Dent Oral Epidemiol. 1996. 24:286–291.
9. Piotrowski BT, Gillette WB, Hancock EB. Examining the prevalence and characteristics of abfractionlike cervical lesions in a population of U.S. verterans. J Am Dent Assoc. 2001. 132:1694–1701.
10. Tyas MJ. The class V lesion - aetiology and restoration. Aust Dent J. 1995. 40(3):197–170.
11. Cuenin M, Clem B. Periodontal and restorative treatment of class V lesion. Gen Dent. 1993. 41:252–254.
12. Litonjua LA, Andreana S, Bush PJ, Tobias TS. Noncarious cervical lesions and abfractions; a re-revaluation. J Am Dent Assoc. 2003. 134:845–850.
13. Grippo JO. Noncarious cervical lesions: The decision to ignore or restore. J Esthet Dent. 1992. 4:55–64.
14. Paolantonio M, D'ercole S, Perinetti G, et al. Clinical and microbiological effect of different restorative materials on the periodontal tissue adjacent to subgingival class V restorations. J Clin eriodontol. 2004. 31:200–207.
15. Larato DC. Influence of a composite resin restoration on the gingiva. J Prosthet Dent. 1972. 28:402–404.
16. Willershausen B, Köttgen C, Ernst CP. The influence of restorative materials on marginal gingiva. Eur J Med Res. 2001. 6:433–439.
17. van Dijken JW, Sjöström S, Wing K. The effect of different types of composite resin filling on marginal gingiva. J Clin Periodontol. 1987. 14:185–189.
18. Blank LW, Caffesse RG, Charbeneau GT. The gingival response to well-finished composite resin restorations. J Prosthet Dent. 1979. 42:626–632.
19. Seibert J, Lindhe J. Linde J, editor. Esthetics and periodontal therapy. Textbook of clinical periodontology. 1989. 2nd edition. Copenhagen: Munksgaard;477–514.
20. Schätzle M, Lang NP, Ånerud Å, et al. The influence of margins of restorations on the periodontal tissues over 26 yers. J Clin Periodontol. 2000. 27:57–64.
21. Jansson L, Blomster S, Forsgårdh A, et al. Interactory effect between marginal plaque and subgingival proximal restorations on periodontal pocket depth. Swed Dent J. 1997. 21:77–83.
22. Goerzo I, Newman HN, Strahan JD. Amalgam restorations, plaque removal and periodontal health. J Clin Periodontol. 1979. 6:98–105.
23. Laurell L, Rylander H, Pettersson B. The effect of different levels of polishing of amalgam restorations on the plaque retention and gingival inflammation. Swed Dent J. 1983. 7:45–53.
 XML Download
XML Download