

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Early generation ceramic articulations were problematic in terms of ceramic implant fracture and wear1-3). Although the mechanical properties of ceramic material have improved during the last three decades, ceramic component fracture remains an issue4). Many authors have reported fractures of the ceramic head5-8), and a few have described ceramic acetabular insert fracture9-11). However, these complications are only encountered rarely, and all cases reported to date involve a history of minor trauma. Here, we describe a case that required 2nd-revision with a CoCr metal head and conventional polyethylene liner due to a recurrent fracture of the ceramic head.
Case report
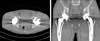
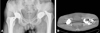
In August 2006, a 44-year-old man(height 180 cm and weight 70 kg) visited our emergency room due to a pain in his left hip. He had not experienced unusual impact or trauma. Previously, he had undergone bilateral primary THA due to avascular necrosis at other university hospital during 2001. The implant used was composed of a hemispherical titanium metal shell and the femoral component was a slightly tapered, rectangular, collarless titanium stem. The proximal one-third of the stem was coated with plasmapore (BiContact, Aesculap, Tuttlingen, Germany), and the articulating component was composed of a ceramic liner and a 28 mm short ceramic head (Biolox Forte, Ceramtec, plochingen, Germany) Although the femoral stem and acetabular cup were well fixed by bony ingrowths, a ceramic fracture was observed on the left side of the ceramic head (Fig. 1). Computed tomography showed an intact liner and broken femoral head in the liner (Fig. 2). Intraoperatively, we observed that the trunion of the femoral stem was not grossly damaged at revision surgery and had a near normal contour. We removed ceramic particular debris carefully and exchanged the head and liner with and a new liner and 28 mm medium neck because of provide stability to the surrounding muscles. The patient followed an uneventful postoperative course (Fig. 3).
However, eight months later, he revisited our emergency room because he felt a 'crunching' sensation in the left hip while walking. Again, he had not experienced any unusual impact or trauma. In the emergency room, we took radiographs of both hips (Fig. 4A). The stem and acetabular cup were still well fixed, but the left side of the ceramic head was fractured and dislocated. Computerized tomographic (CT) scans of both hips revealed metal shells with a normal abduction angle range of 46.14°, but anteversion of the left metal shell was found to be 36.09°(Fig. 4B).
The patient underwent a second revision surgery. Multifragmentary fractured particles of the ceramic head (one on the apical segment and four on the lateral segment) and dark metallic stains were observed on the medial surface of the fractured head. This stain was revealed Ti particles on EDAX study. At the peripheral rim of the ceramic liner, a similar metallic stain and chip fractures were found (Fig. 5A). Interestingly, a groove was observed around the lateral and posterior neck base of the femoral stem (Fig. 5B), indicating impingement between the stem neck and the ceramic liner. During second revision surgery, the fractured ceramic head and the ceramic liner were replaced with 28 mm CoCr medium neck and an elevated-polyethylene liner, which were both replaced anterosuperiorly instead of posteriorly, to overcome excessive anteversion (Fig. 6). The trunion of the femoral stem was retained, although a portion of it was scratched and grooved, because the femoral stem showed bony ingrowth stabilization. Two years after second revision, no postoperative complication or dislocation had occurred, and he was working successfully as a farmer.
Discussion
Alumina ceramic-on-ceramic bearings have been used clinically for more than 20 years6). During these two decades, the mechanical properties of ceramic materials have been improved by hot isocratic pressing, laser marking, and nondestructive proof-testing12). Yet, the risk of fracture remains a major, though fortunately, an uncommon problem. Recently, the majority of reported fractures associated with contemporary third-generation ceramic materials have been chip fractures of ceramic liners13,14), or ceramic liner fractures associated with the use of a sandwich-type acetabular component15).
Patient-specific risk factors that contribute to ceramic component fractures include age, activity level, and a history of trauma10,11). Ha et al.10) attributed ceramic liner fractures in Asian populations to activities, such as, as squatting, kneeling, and sitting cross-legged, which can result in impingement and liner fracture. Our patient was Korean, relatively young, and had no trauma history, but presumably was more active than typical THA recipients.
In terms of operation-associated factors, Barrack et al.1) showed that optimal component positioning is crucial when ceramic-on-ceramic components are used. These components should be placed at less than 45° abduction and 10-15° anteversion on the acetabular side to optimize the distribution of forces over the surfaces of the femoral head and cup1,9,11,16). In our case, abduction and anteversion angles were 46.14° and 36.09°, respectively (Fig. 4). The presumptive cause of the refracture was positioning of the cup in excessive anteversion, which caused impingement between the posterior aspect of the stem neck and the liner followed by subluxation of the head, and head to liner impact due to reduction.
Other possible causative factors of alumina ceramic head fractures include; component design, the material properties of ceramic components, and manufacturing defects, such as, cone-trunion mismatch and ceramic deterioration17-20). The ceramic head to trunion taper contact area is an important aspect of component design, and importantly, a different neck length affects the head-trunion interface. Koo et al.21) showed that fractures involved the thinnest circumferential portions of short necks adjacent to the proximal edge of bore portion of the head, and that several vertical cracks extended from circular cracks to the lower edge of the short neck component. We postulate that the cause of the second ceramic head fracture in our case was not the use of short neck at first revision, but excessive anteversion of metal shell. These recurrent fracture can pose the main cause is the impingement of the metal liner and the base of the neck due to over anteversion of the metal shell followed by ceramic head to liner impact. This postulation is based on the presence of a deep groove in the lateral neck base and a ceramic liner rim fracture. And excessive anteversion of the metal shell on CT scan. On both occasions in our patient, fractures were not associated with trauma and fractures had a brittle fracture pattern. The patient received a 28 mm short neck ceramic head at primary surgery and medium neck at first revision.
Retrieved ceramic femoral heads have shown that metal staining, which appears as dark marks on the inner inferior surfaces of ceramic liners22-24), is caused by metal transfer to the ceramic surface when a head contacts a metal shell during, for example, femoral head reduction or femoral head dislocation11). In our case, metallic staining was observed on the articular surfaces and lips of the ceramic liner, and multiple scratches were the observed on the taper of neck of the retained femoral stem (Fig. 5). Furthermore, EDAX showed that the metal staining on the liner rim was caused by Ti-alloy.
Several options are available for correcting a malpositioned metal shell and a femoral stem with a damaged taper by new implantation of the metal shell and femoral stem with large head or isolated revision on metal shell. We decided to retain all metal components because stable bony ingrowth of the metal shell and femoral component were evident, and thus, we replaced the articular portion only. We choose an elevated polyethylene liner and metal head combination to overcome the damaged taper and to compensate for anteversion of the metal cup. In the present case, during revision, to reduce excessive anteversion, the elevated rim of the polyethylene liner was replaced anterosuperiorly to compensate excessive anteversion and to use 28 mm CoCr metal head on the damaged trunion. After two years of follow up post second revision, our patient was working as a farmer with polyethylene liner and metal head combination THA. However, we cannot conclude that metal shell and femoral stem retentions are optimal in cases of ceramic head fracture. Further studies with longer follow-ups are needed.
Nonetheless, we believe that ceramic-on-ceramic bearings are a good choice for primary THA, especially in young patients. When a hard bearing component as a ceramic head and ceramic liner is used, surgeons should ensure ranges of anteversion and inclination of the metal shell and anteversion of the femoral stem are acceptable.




 XML Download
XML Download