

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
We wanted to assess the clinical results and the complications of treating femoral head fractures.
Materials and Methods
Twenty patients with femoral head fractures and who had a minimum 1 year follow up were enrolled in this study from April 2004 to June 2008. The clinical outcomes were evaluated according to the mechanism of injury, the reduction time, the Pipkin classification, the treatment methods, the surgical approach and the complications.
Results
There were 5 cases of Pipkin type I and 2 cases of Pipkin type II, 1 case of Pipkin type III and 12 cases of Pipkin type IV. All the patients underwent operation except 1 patient; there were 5 excisions, 7 internal fixations, 1 prosthesis, and 6 internal fixations of combined acetabular fixation without surgery for the femoral head fractures. The average Harris hip score at 1 year after operation was 80.0 (range: 57~99): there were 4 excellent, 7 good, 5 fair and 4 poor results. The complications of the femoral head fractures were 2 cases of avascular necrosis and 2 cases of posttraumatic osteoarthritis.
Conclusion
Internal fixation of the femoral head with using Herbert screws showed a favorable outcome, while excision of the femoral head fragments did not. Internal fixation of Pipkin type 1 or 2 fractures could be performed by the anterior approach. The posterior approach combined with surgical dislocation is especially useful in internal fixation of concurrent posterior acetabular fractures, and it has the advantage of preserving the blood supply to the femoral head.
Figures and Tables
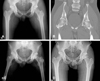 | Fig. 1Case 7. A 36-year-old man (A) Initial both hip Anteroposterior (AP) view and (B) pelvis CT image show Pipkin type 2 femoral head fracture. (C) Internal fixation of femoral head through the anterior approach was done. (D) The last follow-up both hip AP x-ray at postoperative 34 months shows healing of fracture and heterotopic ossification, but there is no evidence of avascular necrosis of femoral head or post-traumatic osteoarthritis.
|
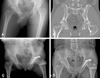 | Fig. 2Case 20. A 48-year-old man (A) Initial both hip Anteroposterior (AP) view and (B) pelvis CT image show Pipkin type 4 femoral head fracture. (C) Internal fixation of femoral head and acetabulum through the posterolateral approach with trochanter flip osteotomy was done. (D) The last follow-up both hip AP x-ray at postoperative 53 months shows healing of fracture, but there is no evidence of avascular necrosis of femoral head or post-traumatic osteoarthritis.
|


References
1. Marchetti ME, Steinberg GG, Coumas JM. Intermediate-term experience of Pipkin fracture-dislocations of the hip. J Orthop Trauma. 1996. 10:455–461.

2. Stannard JP, Harris HW, Volgas DA, Alonso JE. Functional outcome of patients with femoral head fractures associated with hip dislocations. Clin Orthop Relat Res. 2000. 377:44–56.
3. Swiontkowski MF, Thorpe M, Seiler JG, Hansen ST. Operative management of displaced femoral head fractures: case-matched comparison of anterior versus posterior approaches for Pipkin I and Pipkin II fractures. J Orthop Trauma. 1992. 6:437–442.
4. Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res. 1985. 201:9–17.
5. Hougaard K, Thomsen PB. Traumatic posterior fracture-dislocation of the hip with fracture of the femoral head or neck, or both. J Bone Joint Surg Am. 1988. 70:233–239.
6. Lang-Stevenson A, Getty CJ. The Pipkin fracture-dislocation of the hip. Injury. 1987. 18:264–269.
7. Roeder LF Jr, DeLee JC. Femoral head fractures associated with posterior hip dislocation. Clin Orthop Relat Res. 1980. 147:121–130.
8. Sahin V, Karakaş ES, Aksu S, Atlihan D, Turk CY, Halici M. Traumatic dislocation and fracture-dislocation of the hip: a long-term follow-up study. J Trauma. 2003. 54:520–529.
9. Hougaard K, Thomsen PB. Coxarthrosis following traumatic posterior dislocation of the hip. J Bone Joint Surg Am. 1987. 69:679–683.
10. Kim JH, Lee SH, Moon YL, Kim DH, Song KS. Treatment of femoral head fracture with traumatic posterior dislocation of the hip. J Korean Hip Soc. 2007. 19:176–182.
11. Yoo CI, Suh JT, Shin DG. Femoral head fractures associated with traumatic posterior hip dislocations. J Korean Soc Fract. 1991. 4:227–236.
12. Park MS, Rho CK. Clinical analysis of femoral head fracture. J Korean Orthop Assoc. 1992. 27:502–510.
13. Butler JE. Pipkin Type-II fractures of the femoral head. J Bone Joint Surg Am. 1981. 63:1292–1296.
14. Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am. 1957. 39-A:1027–1042.
15. Epstein HC. Posterior fracture-dislocations of the hip; longterm follow-up. J Bone Joint Surg Am. 1974. 56:1103–1127.
16. Ganz R, Gill TJ, Gautier E, Ganz K, Krügel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001. 83:1119–1124.
17. Kloen P, Siebenrock KA, Raaymakers E, Marti RK, Ganz R. Femoral head fractures revisited. Eur J Trauma. 2002. 28:221–233.
 XML Download
XML Download