

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Atrial fibrillation facilitates embolic stroke due to intracardiac thrombus formation caused by increased turbulent blood flow and congestion, and strategies for stroke prevention are the most important issue in patients with atrial fibrillation.1 The Framingham study revealed a fivefold increase in the risk of stroke when atrial fibrillation was present. The average annual rate of ischemic stroke among patients with nonvalvular atrial fibrillation is 5%.2-7 The rate of stroke in atrial-fibrillation patients increases with age and the presence of other risk factors such as a prior stroke or transient ischemic attack (TIA), hypertension, diabetes mellitus, and congestive heart failure.8,9
Since the clotting factor cascade plays a critical role in thrombus formation, warfarin is highly efficacious, and can inhibit effects of the vitamin-K-dependent clotting factors II, VII, IX, and X.10 Although new anticoagulants are about to be introduced, such as dabigatran11 and rivaroxaban, in clinical practice, warfarin has been the only choice for stroke prevention in patients with atrial fibrillation for several decades. However, the levels of warfarin required may vary due to its metabolism by the cytochrome P450 system12 and low efficacy or complications caused by high concentrations in the body such as systemic or intracerebral hemorrhage have also been problematic.13 The prevalence of atrial fibrillation is reported to be up to 10% in the aged population,14 and simple atrial fibrillation may not be associated with the risk of stroke.15 In this context, optimal risk stratification of atrial fibrillation is quite helpful, and the CHADS and CHADS2 (an acronym for congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, and prior stroke or TIA or thromboembolism) scoring systems have been useful for selecting candidate patients who must be treated with warfarin;16-18 although its general application rate has not been high.
It is understood that an increased CHADS2 score is strongly associated with the incidence of recurrent stroke. Therefore, a higher CHADS2 score might be associated with more severe strokes in patients with atrial fibrillation, as well as with worse neurological status and worse long-term prognosis due to worsened quality of life. However, this hypothesis has rarely been tested. In the present study, we investigated how the CHADS2 score is related to stroke severity and long-term outcome in patients with stroke due to atrial fibrillation.
Methods
Study population
Between October 2002 and September 2008, we enrolled a consecutive series of acute ischemic stroke patients with atrial fibrillation who had been admitted to our stroke unit within 7 days after symptom onset (n=339). Patients with other possible potential causes of stroke were initially excluded from the study population by applying the Trial of Org 10172 in Acute Stroke Treatment criteria. From this initial population, we excluded 17 patients whose diagnosis of stroke was not confirmed due to the lack of brain imaging, including magnetic resonance imaging, and further excluded 24 patients without corresponding brain lesions on their brain images. This resulted in 298 stroke patients with atrial fibrillation finally being enrolled in the current study.
All patients received standard medical therapy during and after hospitalization. Collection of the patients' data and recording of all variables were performed prospectively from the beginning of first enrollment by our organized stroke registry system. This study was approved by the local ethics committee [approval no. H-0911-065-301], and complied with the Declaration of Helsinki. Informed consent to participate was obtained from the enrolled patients or their next of kin.
Demographic characteristics and laboratory data
We recorded demographic data (age and gender), conventional risk factors, and important laboratory data for all subjects. Conventional risk factors included hypertension, diabetes, hyperlipidemia, smoking, history of a stroke or TIA, and previous use of antiplatelet or anticoagulant medications. Hypertension was diagnosed if the patients exhibited a systolic blood pressure of >140 mm Hg or a diastolic blood pressure of >90 mm Hg at discharge, or had a previous diagnosis of hypertension and antihypertensive medication use. Diabetes was diagnosed if subjects exhibited a fasting glucose level ≥7.0 mmol/L or had a previous diagnosis of diabetes and antidiabetic medication use. A diagnosis of hyperlipidemia was made in patients with a history of using cholesterol-lowering agents or who had a fasting serum total cholesterol level of >6.0 mmol/L or a low-density lipoprotein cholesterol level of >4.14 mmol/L at admission. Smoking was coded as positive if the patient was a current smoker or an ex-smoker prior to stroke onset. Body mass index was calculated using height and weight values (kg/m2). Fasting blood samples were drawn within 24 hours of admission, and examined for glucose, lipids, and a standard battery of biochemical and hematological tests.
Atrial fibrillation was diagnosed by standard electrocardiography during hospitalization. CHADS2 scoring was performed using the established scoring system, the components of which items are congestive heart failure (1 point), hypertension (1 point), age of 75 years or older (1 point), diabetes mellitus (1 point), and a prior stroke or TIA (2 points).16,17
Neurological severity and mortality
We assessed each patient's clinical state after ischemic stroke with regard to both neurological severity and mortality. First, neurological severity after the stroke was estimated using the National Institutes of Health Stroke Scale (NIHSS) or the modified Rankin Scale (mRS) at discharge. Second, mortality information was obtained from Statistics Korea, a governmental statistics office in South Korea, as at December 2008, as described previously.19-21 The date and cause of death, according to the International Classification of Diseases, 10th Revision, were also recorded.22 Mortality data were classified into vascular death and nonvascular death. Vascular death was defined as death caused by stroke, myocardial infarction, heart failure, pulmonary embolism, cardiac arrhythmia, or other definite vascular causes. Nonvascular death was defined as death caused by nonvascular causes such as accidents, cancer, pulmonary causes (e.g., pneumonia or chronic obstructive pulmonary disease), and other miscellaneous causes.
Statistical analysis
The neurological severity was defined based on the NIHSS or mRS score at discharge. For a severe neurological outcome, we determined the cut-offs as an NIHSS score of 2 or more23 and an mRS score of 3 or more.24 As baseline data, means for continuous variables and proportions for categorical variables were compared using Student's t-test, the Mann-Whitney U test, and Pearson's χ2 test, as appropriate, according to dichotomous classifications of NIHSS or mRS scores. We then reclassified the CHADS2 scores as low risk (0 points), intermediate risk (1 or 2 points), or high risk (3 to 6 points) for comparisons with various variables including neurological severity or mortality.17,18 One-way analysis of variance with the Scheffé post-hoc test and the extended Mantel-Haenszel χ2 for trends were performed to compare the distributions of variables according to each grade of CHADS2 score.
We used a multivariate binary logistic regression analysis test to evaluate neurological severity. To determine whether the power of the association between CHADS2 score and severe neurological outcome was independent of the statistical model setting, we constructed two kinds of multivariate analysis model. In Model 1, together with CHADS2 score, we entered demographic data and conventional risk factors as independent variables, while in Model 2 we further entered clinical variables measured during hospitalization and laboratory variables. In terms of long-term mortality, survival rates after stroke were estimated using the Kaplan-Meier product-limit method, and the survival rates of patients according to CHADS2 score were compared using the log-rank test. To examine the relationship between grade of CHADS2 score and mortality during the follow-up, Cox proportional-hazards regression analysis was used to calculate the crude and adjusted hazard ratios with 95% confidence intervals. Two-tailed p values of <0.05 were considered significant. Data analysis was performed using SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Of the 298 subjects with atrial-fibrillation-related ischemic stroke, 159 were men (53.4%) and 139 were women, and they were aged 69.6±10.2 years (mean±standard deviation). The NIHSS score at discharge was 6.1±8.2, and the number of patients with an mRS score of ≥3 at discharge was 124 (41.6%). Seventy patients (24.1%) died during the follow-up (29.0±20.8 months), with vascular death being the cause in 37 (13.8%). According to CHADS2 score, there were 100, 144, and 54 patients in the high-, intermediate-, and low-risk groups, respectively. Baseline characteristics according to the neurological severity are given in Table 1. Patients with more severe neurological outcomes (NIHSS scores ≥2 or mRS scores ≥3) were more likely to be female, to be older, and to have a greater fasting glucose level at admission. High-risk CHADS2 scores were more common among patients with more severe neurological outcomes.
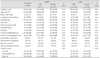
The distributions of demographic and clinical characteristics according to CHADS2 score are given in Table 2. The distributions of age, presence of hypertension, diabetes or congestive heart failure, history of a TIA or stroke, blood glucose level, initial systolic blood pressure, and previous use of antiplatelet agents or anticoagulants differed with the CHADS2 score, as revealed by one-way analysis of variance tests and the extended Mantel-Haenszel χ2 for trends (p<0.05). In terms of neurological outcome at discharge, NIHSS scores were significantly higher in the high-risk group, and the distributions of mRS also differed between the groups. The mortality rate was much higher in the high-risk CHADS2 group, with deaths from all causes and vascular death being 3.8 times (42.9%) and 9.5 times (51.4%) more common, respectively, than in the low-risk group (11.4% and 5.4%, respectively).
The results of the multivariate logistic regression analyses for neurological severity at discharge are given in Table 3. When we used the NIHSS score at discharge to represent the neurological outcome, high-risk patients had a greater risk of a severe neurological outcome (adjusted odds ratio, 4.17; 95% confidence interval 1.76-9.87; reference, low-risk patients) in both Model 1 (adjusted for epidemiological and historical variables) and Model 2 (further adjusted for in-hospital and laboratory variables). In addition, similar results with slightly stronger associations were obtained when we used mRS scores to represent the neurological outcome.
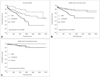
Survival curves are illustrated in Fig. 1. The overall survival among all of the patients differed significantly between the CHADS2 groups, as determined by the log-rank test (p=0.004). Survival from vascular death also differed significantly (p=0.004), whereas that from nonvascular death did not (p=0.18). The crude and adjusted hazard ratios of each CHADS2 group by Cox proportional-hazards regression analyses of death from all causes are listed in Table 4; the low-risk group was used as a reference. The rate of death from all causes was related to CHADS2 score in a stepwise fashion (p for trend=0.006). After adjustment, high-risk CHADS2 scores significantly increased the risk of death from all causes. This trend between CHADS2 groups and death from all causes was also significant (p for trend=0.04). The results for vascular death were similar, with the high-risk CHADS2 score being an independent risk factor and there being a significant dose-response trend (p for trend=0.006).
Discussion
We found that high-risk CHADS2 scores were associated with a worse neurological outcome at discharge and an increased long-term mortality, especially due to vascular causes; it is noteworthy that the associations remained significant after adjustment for in-hospital and laboratory profiles. Since CHADS2 scores can be calculated in individuals even before a stroke event, these results might be useful for estimating future risk of stroke and for designing stroke-prevention strategies for patients with atrial fibrillation.
The CHADS2 scoring system is an algorithm for estimating the risk for embolic stroke in atrial-fibrillation patients, and so higher scores might be associated with an increased amount of thrombus in the heart, which could obstruct larger-sized arteries in the brain and cause more severe neurological damage.25,26 Specifically, a decreased ejection fraction and increased turbulent flow in congestive heart failure will more frequently give rise to a larger thrombus. In addition, hypertension, diabetes, and advanced age have been reported to be associated with increased blood coagulability.27-29 Biochemical markers would reflect the coagulability more precisely in patients with atrial fibrillation.14
Gustafsson et al.30 found that patients with atrial fibrillation had higher concentrations of von Willebrand factor, fibrinogen, D-dimer, and factor VIII. In addition, Lip et al.31 reported a significant correlation between fibrinogen and D-dimer in patients with atrial fibrillation. It was also previously reported that prothrombic markers are related with each component of the CHADS2 score. There was a correlation between hypertension and the level of von Willebrand factor and E-selectin.32 Furthermore, insulin resistance has been associated with plasminogen activator inhibitor-1, von Willebrand factor, coagulation factors VII, VIII, and XII, and fibrinogen. However, it is difficult to apply these biomarkers at the primary hospital level due to poor cost-effectiveness; our strategy using the CHADS2 scoring system might be easier to apply.
One of the strengths of this study is the excellent validity of the mortality information. In Korea, all residents must register their identity information, including the births or deaths of family members, in the Korean Resident Registration System, which has been the only governmental system of the Family Registration Act since 1962. If a family member dies, the other family members must report his or her death with a medical certificate issued by a hospital within 15 days of the death. The death certificate should include information on the exact identification, time, and place of death, and the medical cause of death according to the International Classification of Diseases, 10th Revision. This system is mandatory in Korea, and the statistical results obtained using data from this system have been highly reliable.
In the present study, long-term mortality was clearly improved in patients with high-risk CHADS2 scores. This relationship may be explained by the two assumptions. First, the patients with high-risk CHADS2 scores had multiple vascular risk factors (e.g., hypertension and diabetes). Accordingly, they might have had a higher risk of experiencing vascular events after the onset of stroke, and these multiple recurrent vascular events might aggravate their medical and neurological status, and ultimately increase the risk of mortality during the follow-up. This assumption may be related to the association only being significant for vascular death. Second, we can suggest an explanation of the results related to neurological outcome. The neurological outcomes at discharge (as measured by NIHSS and mRS scores) were more severe in patients with high-risk CHADS2 scores. After discharge, the quality of life of the patients with severe neurological disability must have been poor due to the decreased daily activity and an increased frequency of medical or neurological complications. From a statistical point of view, severe neurological outcome appears to act as a mediator for increased mortality.
There are also some important caveats to this study. First, as mentioned in the Methods section, this study was not designed prior to patient enrollment, although a prospective and consecutive registry system was used, including a variety of demographic, epidemiologic, clinical, and laboratory variables, and all of the components of the CHADS2 scoring system were included in the system. However, we acknowledge that the generalizability of our findings may be limited because this was a single-center study and the most of the included subjects were Korean. Second, we estimated stroke severity using NIHSS and mRS scores "at discharge" instead of the more common time of 3 months after onset. However, a recent report on this issue has indicated that neurological scores at discharge sufficiently represent the final neurological outcome of patients.33 Furthermore, we condensed our data using mortality information. Third, all of the patients included in this study had atrial fibrillation, but in some cases their strokes were caused by other mechanisms such as small-vessel occlusion due to hypertension. We attempted to minimize this limitation by applying the standardized Trial of Org 10172 in Acute Stroke Treatment criteria. Finally, we did not obtain information on compliance to medication course and International Normalized Ratio levels during the follow-up. This limitation could be overcome in a prospectively designed study.
In conclusion, we found that high-risk CHADS2 scores were associated with an aggravated neurological outcome and increased long-term mortality in stroke patients with atrial fibrillation. It might be a natural assumption that the addition of vascular risk factors leads to the occurrence of vascular diseases. Nevertheless, it would be difficult to standardize and estimate the validity of the additive effects of risk factors cannot be easily conducted, and applying an established, validated scoring system is more comprehensive and has a wider potential for application. We believe that our results may be useful for predicting the potential risk of stroke in patients with atrial fibrillation.



 XML Download
XML Download