

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Many epidemiological studies on primary headache disorders have been undertaken since the first edition of the International Classification of Headache Disorders was published in 1988.1 However, the epidemiology of headache disorders in Asian countries remains only partially documented. The reported prevalence of migraine in Asian countries ranges from 1% to 22%, which is lower than the rates reported for North American and European countries.2 Although tension-type headache is the most frequent type of primary headache disorder in the general population, it has only rarely been the subject of epidemiological studies. Moreover, most of these studies were performed in North American and European countries.
The first population-based epidemiological study of migraine and tension-type headache in Korea was conducted in 1995, using telephone interviews and mail surveys.3 That study found prevalence rates of migraine and tension-type headache of 22.3% and 16.2%, respectively. The prevalence of migraine was extraordinarily high, while that of tension-type headache was lower than in other Asian countries. In the present study we conducted a detailed, semistructured, face-to-face survey to verify the previously reported results for the prevalence rates of migraine and tension-type headache in Korea.
The major objectives of this study were to estimate the 1-year prevalence rates of migraine and tension-type headache in a Korean population, based on the second edition of the International Classification of Headache Disorders (ICHD-2). We also investigated the impact of headaches among migraineurs and individuals with tension-type headache.
Methods
This study was a nationwide, cross-sectional, descriptive survey of primary headache disorders in a Korean population. Structured interviews were conducted using a questionnaire to determine the status of headache disorders in adults aged 19 years or over by trained interviewers. The survey included items on the symptoms, management, and impact of headache. The socioeconomic, demographic, and geographic factors of the participants were also evaluated. This study was performed in March 2009 in accordance with the ethical guidelines of the Council for International Organizations of Medical Sciences,4 and the principles in the Declaration of Helsinki.5
Target area
Korea is divided geographically into 15 administrative divisions ("do"), which with the exception of Jeju-do are further divided into 3 basic administrative units: "si", "gun", or "gu"; there are 77 si, 88 gun, and 69 gu. According to data from the 2005 population and housing census from the National Statistical Office, the estimated population of Korea in 2009 was 49759141, of which approximately 37394000 people were aged 19 years or over.6 This study included all Korean territories except Jeju-do. We classified seven metropolitan "si" areas (Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, and Ulsan) as "big cities", other "si" areas as "middle-sized or small cities", and "gun" areas as "rural areas" for the analysis.
Sampling method
To obtain prevalence rates and analyze the demographic factors affecting common primary headache disorders, we planned to sample 1500 individuals based on the population structure. A 2-stage systematic random sampling method was adopted, and the 15 administrative divisions were designated as the primary sampling units. Appropriate sample numbers were assigned at each primary sampling unit according to the population distribution. In the second stage, we further selected representative basic administrative units (si, gun, and gu) for each primary sampling unit. Overall, 60 representative basic administrative units were selected for this study, in each of which we assigned a target sampling number regarding age, gender, and occupation. The estimated sampling error of our study was ±2.5%, with a 95% confidence interval (Table 1).7
Questionnaire
The questionnaire comprised three parts. The first part assessed demographic and socioeconomic characteristics (9 questions), the second part established a headache profile, which was designed to comply with ICHD-2 criteria (13 questions), and the third part involved questions about headache management including recognition of headache diagnosis, use of medical services for headache, and headache treatment (6 questions). We also included the Headache Impact Test-6 questionnaire (HIT-6)8 to evaluate the impact of headache on the sufferer's life.
Diagnosis of migraine and tension-type headache
Migraine was diagnosed according to ICHD-2 diagnostic criteria.9 The diagnosis of migraine in this study required the experience of five or more attacks in a lifetime, with each attack lasting 4-72 hours and accompanied by any two of the following four pain characteristics: unilateral location, pulsating quality, moderate-to-severe intensity, and aggravation by routine physical activity. In addition, the attacks must have been associated with at least one of the following: nausea or vomiting, or both photophobia and phonophobia. The diagnosis of tension-type headache was also made using ICHD-2 diagnostic criteria. We included only subjects who had experienced ten or more attacks in a lifetime that had lasted from 30 minutes to 7 days each and were accompanied by at least two of the following four pain characteristics: bilateral location, non-pulsating quality, mild-to-moderate intensity, and nonaggravation by routine physical activity. Associated symptoms could not include nausea or vomiting, but could include either photophobia or photophobia, but not both.
Impact of headache
We included the validated Korean version of the HIT-6 test in the questionnaire to assess the impact of headache.8 The HIT-6 test is a tool used to measure a wide spectrum of the impact of headache, including migraine and tension-type headache, on individuals who experience them. The HIT-6 score was used to assign the subjects an impact grade as follows:10,11 36-49, no impact; 50-55, some impact; 56-59, substantial impact; and 60-78, severe impact.
Survey procedures
Our interviewers interviewed their assigned and numbered participants (aged ≥19 years), who were stratified according to age, gender, and occupation, after explaining to them the study objectives and methods. Before the initial face-to-face interviews, the interviewers were told 1) the aims of the present study, 2) the meaning of each question, 3) to check the participants' responses, and 4) other details relevant to conducting a proper interview.
Validation of migraine and tension-type headache diagnoses
We assessed the validity of migraine and tension-type headache diagnoses by comparing them with those of neurologists in an additional telephone interview. At the initial interview, we asked all participants whether they would agree to an additional telephone interview with neurologists. If they agreed, they participated in an additional telephone interview with nine doctors (eight neurologists and one dentist; see acknowledgements) within 2 weeks of the initial face-to-face interview.
Analyses
Unless noted otherwise, the diagnosis of migraine and tension-type headache was based solely on ICHD-2 criteria. Based on this diagnosis, the 1-year prevalence with 95% confidence interval is presented as the number of cases per 100 persons. Age- and gender-specific prevalence rates were also calculated. The results were analyzed using statistical software for Windows version R 2.9.1 and R commander 1.4-10 (The R foundation, GNU general public license). Student's t-test, chi-square test, and analysis of variance were used for comparisons when appropriate. The level of statistical significance was set at p<0.05.
As with most survey sampling designs, missing data resulting from nonresponse occurred for several variables. The reported data are based on the available data. Sample sizes for variables that diverged from the sample size of n=1507 are attributable to nonresponses for that particular variable. Imputation techniques were not employed to minimize nonresponse effects.12
Results
Survey
Our 76 interviewers completed semistructured, face-to-face interviews with 1507 participants in the present study. Each interviewer interviewed 9-35 participants.
Headache
Prevalence of headache
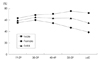
Of the 1507 participants, 926 (61.4%) reported having had a headache at least once during the previous year. The prevalence of headache was significantly higher in women (70.0%) than in men (52.7%; p<0.001). The prevalence of headache among different age groups was highest in the fifth decade for women and in the third decade for men (Fig. 1). The prevalence of headache did not differ among the 15 administrative divisions in Korea, and ranged from 54.7% to 73.3% (p=0.419) (Table 1).
Impact of headache
Among the participants who reported any headache in the previous year, 632 (68.3%) reported that they had had little or no impact (HIT-6 score ≤49), 170 (18.3%) reported some impact (HIT-6 score 50-55), 55 (5.9%) reported substantial impact (HIT-6 score 56-59), and 69 (7.5%) reported severe impact (HIT-6 score ≥60) (Fig. 2A).
Migraine
Prevalence of migraine
Of the 1507 participants, 92 (6.1%) were classified as having had at least 1 migraine during the last year. The women-to-men ratio was 3.2 : 1 (women, 9.2%; men, 2.9%). The prevalence of migraine was highest in females aged 40-49 years and in males aged 19-29 years, although this prevalence subsequently decreased with age (Fig. 3). The prevalence of migraine was inversely associated with the size of the place of residence (p=0.002). The prevalence of migraine did not differ significantly with the monthly income and the education level (Fig. 4).
Impact of migraine
Of the 92 participants classified as having had at least 1 migraine in the previous year, 39 (42.8%) reported that it had had little or no impact, 23 (25.7%) reported some impact, 12 (13.0%) reported substantial impact, and 17 (18.5%) reported severe impact (Fig. 2B).
Tension-type headache
Prevalence of tension-type headache
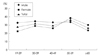
Of the 1507 sampled participants, 464 (30.8%) were classified as having had at least 1 tension-type headache during the previous year. The 1-year prevalence of tension-type headache did not differ significantly between men and women (32.5% vs. 29.1%; p=0.159). Although the prevalence of tension-type headache was highest in the 50-59 year age group, it did not differ markedly with gender or age (Fig. 5). The education level, size of the place of residence, and monthly income did not affect the prevalence of tension-type headache (Fig. 6).
Impact of tension-type headache
Among the 464 participants who were classified as having tension-type headache, 366 (78.9%) participants reported that it had had little or no impact, 65 (14.0%) reported some impact, 18 (3.9%) reported substantial impact, and 15 (3.2%) reported severe impact (Fig. 2C).
Validation of migraine and tension-type headache diagnosis
Overall, 135 of the 1507 participants agreed to an additional telephone interview for validation of their headache diagnosis, and 82 of them completed the telephone interview. The sensitivity and specificity were 75.0% (36/48) and 88.2% (30/34), respectively, for migraine diagnosis, and 86.2% (25/29) and 75.5% (40/53) for tension-type headache diagnosis. The diagnoses of migraine and tension-type headache did not differ significantly between the nine neurologists. The failure of headache diagnosis by telephone interview was attributable to 1) inability to access participants, 2) refusal to submit to an additional interview, and 3) inappropriate responses during the additional interview.
Discussion
The present study confirms that headache is a common problem in the Korean adult population, with 1-year prevalence rates of 61.4% overall and 6.1% and 30.8% for migraine and tension-type headache, respectively. Approximately 13.4% of all headache sufferers, 31.5% of migraineurs, and 7.1% of individuals with tension-type headache were either substantially or severely impacted by the headache.
Epidemiological data on migraine are available for six eastern and southeastern Asian countries: Hong Kong,13,14 Malaysia,15 Japan,16,17 Korea,3 Singapore,18 and Taiwan.19 The Singapore study documented only the lifetime prevalence rates of migraine; the 1-year prevalence rates in the remaining five countries varied widely, from 1%14 to 22.3%.3 The wide range of prevalence rates in these studies might be related to methodological differences between the studies, discrepancies in the interpretation of ICHD-2 in different languages, differences in sociocultural backgrounds, and genetic factors. However, except for the previous report for Korea and the first report for Hong Kong, the 1-year prevalence of migraine in Asian countries has been fairly consistent, ranging from 4.7% to 9.1%,13,15-17,19 and is lower than that of European (10-25%) and North American (9-16%) countries.2
The first nationwide epidemiologic study of migraine in Korea was conducted in 1995.3 The 1-year prevalence of migraine found in the first study was 22.3%, which is almost four times higher than that found in the present study. This large discrepancy could be due to several factors. First, while most previous studies of migraine prevalence excluded probable migraine (ICHD-2 code 1.6), it was included under the diagnosis of migraine in the first study. The prevalence of migraine was 17.5% in our study if both migraine and probable migraine were included. Second, the low response rates for both the telephone (68.3%) and postal (41.0%) surveys may have introduced interest bias and led to artificially high estimates of prevalence rates. Third, the difference may reflect sociocultural change in Korea, whereby industrialization and economic development have increased dramatically since the first study. Finally, the first study is the only epidemiological study in which the prevalence of migraine (22.3%) surpassed that of tension-type headache (16.2%), suggesting the presence of misclassification in that study.
Migraine was about three times more common in women (9.2%) than in men (2.9%) in our study. The prevalence was highest in women aged 40-49 years and men aged 19-29 years. The ratio between men and women for migraine prevalence was similar to that in previous studies employing a variety of methodologies.20-22 While migraine prevalence peaked at the age of 30-40 years for women and at around 30 years for men in most studies from Western countries,20,21,23 our findings were similar to studies from Asian countries. A population-based study from Japan found that the prevalence of migraine was highest in the fourth decade of life in women and in the second decade in men.17 In Taiwan, the prevalence peaked in the second decade in men and in the third decade in women.19 The prevalence of migraine among women in their 40s was similarly high in the present study. In Hong Kong, the migraine prevalence peak at 45-54 years of age in men and at 25-34 years of age in women.13 The distribution of age- and gender-specific prevalence rates of migraine in our study might reflect the importance of hormonal influences in the development of migraine across the lifespan.
It is notable that the prevalence of migraine was influenced by socioeconomic variables. The reported migraine prevalence has generally been inversely related to socioeconomic status. However, studies conducted outside the United States have not consistently confirmed an inverse relationship between migraine prevalence and household income. "Rural residence" and "lower education level" increased the prevalence of migraine. Although the prevalence did not differ markedly with monthly income in the present study, "lower income" factors associated with low socioeconomic status, such as stress, poor diet, or limited access to medical care, act to increase the migraine prevalence. The reasons for the migraine prevalence varying with socioeconomic status are still not clear. In physician- and clinic-based studies, migraine appears to be associated with high intelligence and social class.23 However, data from general population studies do not indicated an increased prevalence in more privileged or educated societies.24
While tension-type headache is the most common headache disorder in the general population, nationwide studies of tension-type headache have been conducted in only four countries: Korea,3 Canada,25 Germany,26 and Brazil.27 Two of these studies were conducted by telephone interview.3,25 The prevalence of tension-type headache was 36% in Canada,25 38.3% in Germany,26 16.2% in Korea,3 and 13% in Brazil.27 In the present study, the 1-year prevalence of tension-type headache was 30.8% (32.2% in men and 29.3% in women), which is comparable with the findings of previous studies.25,26
The increased prevalence of migraine among women is consistent across studies; however, gender difference is not marked in tension-type headache in most countries.2 Unlike migraine, the prevalence rates of tension-type headache did not differ between different age groups or between genders in the present study; hormonal influence may thus be less important in the development of tension-type headache.
During headache attacks, individuals with headache were being impacted by headache via, for example, pain, decrease in functioning, psychological distress, and decreased vitality.10,28 The overall impact of headache is to decrease the sufferers' quality of life. The HIT-6, a self-reported scale, was used to assess the impact of headache in individuals in the present study. If a headache sufferer is being substantially or severely impacted, as evidenced by their HIT-6 score, he/she may experience a significant decrease in quality of life due to their headaches.11,28
In the present study, 31.5% of migraineurs, 7.1% of individuals with tension-type headache, and 13.4% of all headache sufferers were being substantially or severely impacted by their headache, as assessed by the HIT-6 test. Considering the prevalence and the proportions of participants who were substantially-to-severely impacted by headache, approximately 3.8%, 2.2%, and 8.3% of the Korean population experience significant decreases in quality of life due to migraine, tension-type headache, and all types of headache, respectively.
This study has revealed the 1-year prevalence rates and the impact of the two most common headache disorders in a Korean population. However, these findings should be interpreted in the light of several study limitations. First, our study was a cross-sectional survey conducted by semistructured interview using a questionnaire; recall bias may thus have affected the prevalence rates of the headache disorders. However, the 1-year prevalence rates are less likely to be subject to recall bias than the lifetime prevalence rates found in other studies. To minimize recall bias, we investigated only subjects who reported headaches within the previous year. In addition, no attempt was made to investigate the presence of aura in the present study because the diagnosis of aura is very difficult to document using the questionnaire method.29 ICHD-2 criteria for migraine with aura are not only difficult to translate into a questionnaire or an interview, but are also too vague to interpret.
Second, we used the HIT-6 test to assess the impact of headache. HIT-6 is an instrument that is used to assess the impact of headache on individuals.11,28 However, headache impacts not only the individuals themselves, but also society through, for example, decreased productivity, absence from school and work, and use of medical services.2,20 Unfortunately, the HIT-6 test cannot assess the social impact of headache, and as a result we could not investigate the social impact of headache in the present study.
Third, although the present study had a population-based design with a low sampling error, the statistical power was limited for examining subgroups. Thus, some conditions that did not reach statistical significance could merely be a reflection of the small samples.
Fourth, we assessed the validity of migraine and tension-type headache diagnosis by comparing the headache diagnoses of neurologists with an additional telephone interview. We asked all participants to take part in an additional telephone interview, but only a small proportion of them completed that interview. However, the sensitivity and specificity of the diagnoses were substantial and we were able to confirm that the diagnoses of migraine and tension-type headache were appropriate in the present study. The high prevalence of migraine among telephone interviewees may be due to their interest bias because of the severe headache symptoms experienced by migraineurs.
This is the first nationwide, population-based, face-to-face survey of all headaches and of migraine and tension-type headaches in the Korean population. The prevalence rates of all headaches and of migraine and tension-type headaches were 61.4%, 6.1%, and 30.8%, respectively. While the prevalence of migraine in Korea is lower than those in Western countries, it is similar to those in other Asian countries. The findings regarding the impact of headache suggest that approximately one-third of migraineurs and a smaller proportion of individuals with tension-type headache experience a significant decrease in quality of life due to headaches.





 XML Download
XML Download