

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Strokes are more severe, cause greater disability, and have worse outcomes in individuals with atrial fibrillation (AF) than in individuals without AF.1,2 Nonvalvular AF (NVAF) is associated with a fivefold increase in the risk of stroke, and stroke associated with this condition accounts for approximately 15% of all strokes.3 Moreover, the likelihood of developing NVAF increases with age.4 It is therefore important to minimize the risk of stroke in patients with NVAF.
Oral anticoagulant therapy can prevent thromboembolic events, but such therapy increases the risk of bleeding. Therefore, stroke risk-stratification schemes have been proposed to identify high-risk patients among individuals with NVAF. Stroke Prevention in Atrial Fibrillation III (SPAF-III) investigators have reported that the incidence of thromboembolism is correlated with the presence of transesophageal echocardiography (TEE) risk markers in patients with NVAF.5 Moreover, the National Registry of Atrial Fibrillation reported that CHADS2, a stroke risk index, could be used to quantify the risk of stroke in patients with NVAF, and perhaps even aid in the selection of antithrombotic therapy.6 It has been confirmed that CHADS2 is statistically significantly associated with the risk of stroke. However, in the clinical setting, whether the CHADS2 index is the most relevant among the various existing indices for evaluating the risk of stroke in individual patients remains to be determined. The aim of the present study was therefore to clarify which factors among not only the baseline clinical characteristics (including the CHADS2 risk factors), but also echocardiographic findings might most accurately predict the risk of stroke in patients with NVAF.
Methods
Study population
TEE was performed in 745 patients with AF who were admitted to our department at Toyama University Hospital (Toyama, Japan) between November 1994 and May 2007 for the management of cardiovascular disease. TEE is routinely performed in patients admitted to our department with AF in order to determine the risk of future embolic events. However, it is not performed in patients in the acute phase of cardiovascular events, including ischemic stroke or myocardial infarction, or in those suffering from infection or critical illness. Ultimately, 608 patients (82%) were enrolled for the present study after obtaining their written consent to participate. This retrospective study was conducted with the approval of the Toyama University Ethics Committee.
Among the 608 patients with AF, 82 had valvular AF and 526 had NVAF. TEE was performed in all of the NVAF patients, but technically adequate TEE data were not obtained from 36 patients. Therefore, only the data from the remaining 490 patients (men : women=357 : 133; age 67±11 years, mean±SD) were included in the analysis for the present study. The following baseline clinical characteristics parameters were determined from the medical records: including age, gender, presence/absence of recent congestive heart failure, hypertension, diabetes mellitus, and history of cerebral ischemia, the CHADS2 score, history of antiplatelet therapy or anticoagulant therapy with warfarin, and the prothrombin time-international normalized ratio (PT-INR). Routine laboratory data were also determined from the medical records.
Echocardiography
Transthoracic echocardiography was performed using an ultrasound imaging system. The left atrial dimension (LAD), left ventricular diastolic dimension, and the left ventricular ejection fraction (LVEF) were determined from the M-mode images.
TEE was performed with a 5-MHz multiplane transducer connected to an ultrasound system. Each patient was studied in the fasting state without premedication. Multiple standard tomographic planes were imaged. The left atrial appendage peak flow velocity (LAAPV), presence of thrombi in the left atrium (LA), and severity of spontaneous echo contrast (SEC) in the LA (LASEC) were determined. LA appendage flow-velocity profiles were obtained by pulsed-wave Doppler echocardiographic imaging at the orifice of the appendage. The peak outflow velocity signals within each R-R interval were averaged over a minimum of six cardiac cycles. Atrial cavity or appendage thrombi were considered to be present when well-circumscribed, echodense, intracavitary masses that were acoustically distinct from the underlying endocardium and pectinate muscles were identified. LASEC was diagnosed in the presence of dynamic smoke-like echoes within the LA, and its severity was defined using the criteria of Fatkin et al.7 Aortic plaques were classified as either simple or complex (with the latter defined as any combination of mobile, pedunculated, and ulcerated morphologies, or a plaque thickness of ≥4 mm).8
LA abnormality was defined as a slow LAAPV (less than 20 cm/sec) and/or the presence of LA thrombi or dense LASEC (≥grade 3+). Aortic atherosclerosis was defined as the presence of complex aortic plaques. According to the SPAF-III study, TEE risk was defined as the existence of LA abnormality and/or aortic atherosclerosis.5
The LAAPV, presence of LA thrombi, severity of LASEC, and presence of complex aortic plaques were determined by two independent observers (K.N. and T.H.). Any differences in the image interpretation were resolved by the opinion of a third observer (K.O.).
Outcomes
The composite endpoints of death from any cause, ischemic stroke or systemic embolism, and cardiac events (myocardial infarction or hospitalization for worsening heart failure) were determined in October 2008. Information on the endpoints was collected from the hospital databases and responses to questionnaires by the patients themselves or their family mem-bers. Stroke was defined as sudden onset of neurological deficit lasting for >24 hours. Whether a stroke was ischemic or hemorrhagic was confirmed by brain computed tomography and/or magnetic resonance imaging. Our evaluation of the incidence of ischemic stroke or systemic embolism indicated that none of the patients had a symptomatic systemic embolism.
Statistical analysis
Data are expressed as either mean±SD or percentage values. All analyses were performed using SPSS software (SPSS 11.0J, Chicago, IL, USA). The mean values and proportions of variables were compared by the nonpaired t-test for continuous variables and the χ2 test for categorical variables. The outcomes were assessed using Kaplan-Meier survival curves and compared using the log-rank test. Cox proportional-hazards regression analysis was used to identify independent predictors of ischemic stroke. The level of statistical significance was set at p<0.05.
Results
Among the 490 patients with NVAF who were enrolled in this study, 143 (29%) died, 89 (19%) had cardiac events (11 with myocardial infarction and 78 hospitalized for worsening heart failure), and 42 (9%) developed ischemic stroke during the follow-up period (5.7±3.3 years). None of the patients had symptomatic mesenteric or peripheral emboli. In the present study, the ischemic stroke risk was estimated to be 1.5% per year. On the other hand, ten of the patients (2% of the entire cohort) had hemorrhagic stroke, of which nine were on warfarin therapy. Therefore, the risk of hemorrhagic stroke was estimated to be 0.46% per year in patients on warfarin therapy. Table 1 compares the clinical characteristics and echocardiographic markers in the patients showing subsequent development/no development of ischemic stroke. On average, the patients who suffered from ischemic stroke were older (p<0.001) and were more likely to be 75 years old or over (p<0.01) relative to the patients that did not develop ischemic stroke events. The frequency of warfarin use, PT-INR, and transthoracic echocardiographic findings did not differ significantly between the two groups. Although the prevalence rates of LA abnormality and aortic atherosclerosis also did not differ between the two groups, the prevalence of TEE risk was significantly higher in the ischemic stroke group than in the stroke-free group (p<0.01).
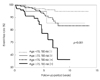
As shown in Fig. 1A, the incidence of ischemic stroke was significantly greater in patients with CHADS2 scores of ≥2 (p<0.05). Table 2 lists the results of the univariate analyses using Kaplan-Meier curves to identify the risk factors for ischemic stroke events. According to the univariate analyses, age ≥75 years (p<0.001), a history of cerebral ischemia (p<0.05), a CHADS2 score of ≥2 (p<0.05), and the presence of TEE risk (p<0.001, Fig. 1B) were significantly positively correlated with the incidence of ischemic stroke.
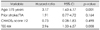
Cox proportional-hazards regression analyses identified age ≥75 years [hazard ratio (HR), 3.17; 95% confidence interval (CI), 1.63-6.17; p<0.01] and the presence of TEE risk (HR, 2.96; 95% CI, 1.33-6.57; p<0.01) as significant predictors of ischemic stroke in patients with NVAF, after adjustments for a history of cerebral ischemia and CHADS2 score (Table 3).
The predicted annual ischemic stroke event rates based on a combination of age and presence/absence of TEE risk are given in Table 4. The rate of ischemic stroke events was significantly higher in persons who were 75 years of age or older with TEE risk than in persons under 75 years of age without TEE risk (4.3% vs. 0.56% per year; adjusted HR, 8.94; 95% CI, 3.44-23.28; p<0.001). The adjusted HRs for ischemic stroke were comparable for those who were younger than 75 years but had TEE risk and those who were 75 years old or older without TEE risk (Table 4, Fig. 2).
Discussion
Whether the CHADS2 index might be the most useful of the various indices for evaluating the risk of stroke in individual patients in the clinical setting remains to be elucidated.9-11 In order to reevaluate the risk of stroke in patients with NVAF, we examined the long-term incidence of ischemic stroke in 490 patients with NVAF who had undergone TEE at our hospital. Our findings demonstrate that while the ischemic stroke rate was significantly correlated with the CHADS2 score, the presence of TEE risk was also significantly correlated with the incidence of ischemic stroke. These results are consistent with those of previous studies.5,7 Cox proportional-hazards regression analyses identified age ≥75 years and presence of TEE risk as significant independent predictors of ischemic stroke events in patients with NVAF. Moreover, the risk estimation for ischemic stroke was more accurate for the combination of age and TEE risk than for the CHADS2 score. Thus, our results indicate that TEE findings might be more relevant predictors of ischemic stroke than the CHADS2 score in patients with NVAF, and that the stroke risk was more than eightfold higher in patients aged ≥75 years with TEE risk.
In fact, thromboembolism could occur even in patients with low CHADS2 scores. Kleemann et al.12 reported that 3% of their patients had LA thrombi and 8% had dense SEC despite having a low CHADS2 score of 0 or 1, and that the independent predictors of the presence of LA thrombi and dense SEC were an LVEF of <40% and an LAD of ≥50 mm. They concluded that echocardiography might be a useful tool for risk stratification in patients with low CHADS2 scores. On the other hand, in a subgroup analysis of the SPAF-III study, 382 patients with AF at high risk for thromboembolism underwent TEE at 18 echocardiography laboratories, and the correlation of the TEE findings with the subsequent development of ischemic stroke events was evaluated prospectively over a mean follow-up period of 1.1 years. The authors concluded that the subsequent occurrence of thromboembolism in the patients with AF was correlated with the presence of dense SEC, thrombus in the LA appendage, and/or aortic plaques.5 Thus, based on the results of the present study, it was concluded that the presence of TEE risk might serve as an independent predictor of ischemic stroke in patients with NVAF.
While the severity of blood stasis in the LA and presence of aortic atherosclerosis have been reported to be correlated with an accumulation of clinical risk factors for thromboembolism in NVAF patients,13,14 the results of the present study suggest that the CHADS2 score alone is not sufficient to predict the risk of ischemic stroke. The existence of complex aortic plaques is considered to be a marker of atherosclerosis, and is known to enhance hypercoagulability in patients with NVAF.15 Therefore, the development of an accurate ischemic stroke risk stratification scheme that would include certain types of laboratory data such as TEE risk markers that directly reflect a prothrombotic condition of the LA is warranted.16,17
The invasiveness and requirement for operator proficiency of the TEE examination make it desirable to develop alternative less-invasive tools that are at least as reliable as TEE. Kleemann et al.12 reported that LVEF and LAD on transthoracic echocardiography were independent predictors of the presence of thrombus in the LA and dense SEC on TEE, whereas the present study found that transthoracic echocardiographic markers were not significantly associated with these factors. Thus, further studies are warranted to evaluate the correlation between LVEF and LAD, and the presence of TEE risk. The addition of hemostatic markers, such as D-dimer levels, to the criteria for stroke risk stratification should also be considered.15,18,19
The ischemic stroke rate was 1.5% per year in the present study, which is slightly higher than that found in previous trials in which warfarin therapy was adjusted to maintain the PT-INR at 2-3. Japanese guidelines recommend low-intensity adjusted-dose warfarin with a target PT-INR of 1.6-2.6 for NVAF patients aged 70 years or over.20 The mean PT-INR of 1.7 in the present study indicates that the treatment in most patients was consistent with those guidelines. Although warfarin evidently reduces the risk of stroke in patients with NVAF, there are ethnic and racial differences in the risk of intracranial hemorrhage with warfarin treatment that should also be taken into consideration.21 In the present study, the rate of warfarin use or PT-INR did not differ between patients with and without subsequent development of ischemic stroke. According to a Kaplan-Meier curve analysis, warfarin therapy was not associated with any significant reduction in the incidence of stroke. The present study had an observational rather than a randomized design, and more than 70% of the patients were receiving warfarin therapy according to the judgment of the attending physician. Therefore, the CHADS2 scores appeared to be higher in the patients on warfarin therapy (1.60±1.37) than in those not on warfarin therapy (1.45±1.38), although the difference was not statistically significant. Moreover, the percentages of patients with a history of congestive heart failure and with LA abnormality were significantly higher for those on warfarin therapy (26% and 42%, respectively) than for those not on warfarin therapy (12% and 28%), which made it difficult to evaluate the reduction in stroke occurrence related to warfarin therapy from the data obtained in the present study.
Hart and Pearce11 described several problems related to stroke risk stratification schemes for NVAF patients. Even NVAF patients with low CHADS2 scores may occasionally develop ischemic stroke events. In addition, it is necessary to consider the prevention of stroke recurrence in patients on warfarin therapy who develop an ischemic stroke. The results of the present study actually indicate that TEE risk might be a powerful independent predictor of ischemic stroke in individual patients with NVAF, and that the stroke risk was greater than eightfold higher in patients aged ≥75 years with TEE risk. Furthermore, a patient with TEE risk may develop an ischemic stroke even if he or she is on usual-dose warfarin therapy. Therefore, high-intensity warfarin therapy or treatment with a direct thrombin inhibitor should be considered in patients with TEE risk.
The present study was subject to several limitations. First, the study had a retrospective rather than a prospective design. Second, the inclusion of a relatively small sample from one institution might have affected the statistical power of the analyses. Third, 70% of the patients were on warfarin therapy according to the judgment of the attending physician, and the status of treatment with antithrombotic drugs was not determined systematically throughout the follow-up period. Finally, selection bias might have been present, since the subjects were selected from among patients with NVAF who had undergone TEE for evaluation of the potential risk of thromboembolism. This meant that the present study involved NVAF patients who already had a comparatively high risk of developing thromboembolic events.
Despite the aforementioned limitations, the results of the present study indicate that the presence of TEE risk may be a powerful and independent predictor of ischemic stroke events in individual patients with NVAF. Although the CHA2DS2-VASc score has recently been proposed,16 the present results suggest that certain parameters directly indicating a prothrombotic state in the LA should be added to any ischemic stroke risk stratification scheme for individual patients with NVAF. We believe that a prospective study should be performed in the future to confirm the results of our present study.




 XML Download
XML Download