

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Charcot-Marie-Tooth disease (CMT) is the most common hereditary motor and sensory neuropathy, and CMT type 1A (CMT1A) neuropathy, which is the most common type of CMT, is subject to a gene dosage effect.1 The primary genetic cause of CMT1A is a duplication of PMP22 resulting from the unequal crossover between two homologous repetitive elements that flank the 1.4-Mb region of chromosome 17p12.2 A new mechanism responsible for the outbreak of CMT1A-which is related to a nonrecurrent rearrangement has recently been reported.3 CMT1A is also caused by a point mutation in PMP22.4
Abnormal axon-Schwann cell interactions cause abnormalities in axonal structure and function, but the exact pathogenic mechanism causing CMT1A is unknown.5 One obvious possibility is that the weakness and sensory loss are the result of axonal degeneration; secondary axonal degeneration is common in CMT1A patients, and its degree determines the patient's functional disability.6 This finding is consistent with the electrophysiological and clinical findings in patients with CMT1A and in several animal models of demyelinating neuropathy.7,8
Axonal dysfunction induced by demyelinating Schwann cells can also occur without axonal degeneration.9 The relationship between motor nerve conduction velocities (MNCVs) and disease disabilities has been the subject of much debate.10-14 Most CMT1A research groups have found a relatively weak correlation between the severity of muscle weakness and nerve conduction velocities,10-12 although some have noted that patients with slower velocities developed more weakness.13,14 Moreover, longitudinal studies have shown that the velocities remained unchanged over decades, whereas the compound muscle action potential (CMAP) amplitudes decreased.15,16 However, the relationship between MNCVs, CMAPs, and the disease severity has not been investigated in Koreans. Therefore, we determined whether there is a correlation between clinical disabilities and electrophysiological values in Korean CMT1A patients with PMP22 duplication.
Methods
Patients
We enrolled 167 CMT1A patients (93 males, 74 females) with PMP22 duplication who took part in nerve conduction studies at 20 university hospitals in Korea. We excluded CMT1A patients with a partial duplication or a PMP22 point mutation. All of the participants provided written informed consent to participate. This study was approved by the Institutional Review Board of the Ethics Committee of the Ewha Womans University Hospital.
Clinical assessments
The patients' clinical information was obtained and analyzed, including assessment of the gender ratio, age at onset, disease duration, motor and sensory impairment, deep tendon reflex, and muscle atrophy. The age at onset was determined by asking the patients when their symptoms-such as distal muscle weakness, foot deformity and/or sensory change-first appeared. Sensory impairments were determined according to the severity of pain and vibration. The impairment and progression of CMT was evaluated in these patients using two scales: the functional disability scale (FDS)13 and the CMT neuropathy score (CMTNS).17 Disease severity was quantified for each patient using a 9-point FDS based on the following criteria: 0, normal; 1, normal but with cramps and fatigability; 2, unable to run; 3, difficulty walking but still able to walk unaided; 4, walking with a cane; 5, walking with crutches; 6, walking with a walking frame; 7, wheelchair bound; and 8, bedridden. In addition, we determined the CMTNS based on the motor and sensory symptoms, and according to the pain and vibration, muscle strength, and neurophysiologic test results. The scores of this test were used to divide the patients into two groups: mild (0<CMTNS≤10) and moderate or severe (CMTNS≥11).
Electrophysiological studies
The MNCVs and sensory nerve conduction velocities (SNCVs) for the median, ulnar, peroneal, tibial, and sural nerves were determined in all 167 patients. The recordings were obtained by standard methods using surface stimulation and recording electrodes. The MNCVs of the median and ulnar nerves were determined by stimulating at the elbow and wrist, respectfully, while CMAPs were recorded over the abductor pollicis brevis and the adductor digiti quinti, respectively. The MNCVs of the peroneal and tibial nerves were determined by stimulating at the knee and ankle while recording the CMAPs over the extensor digitorum brevis and adductor hallucis, respectively. The SNCVs and sensory nerve action potentials (SNAPs) were obtained over a finger-wrist segment from the median and ulnar nerves, and they were also recorded for the sural nerves.
The terminal latency indices (TLIs) that adjust the distal motor latency for the terminal distance and the proximal MNCV were calculated. The calculated TLI was compared to the TLI of the normal population as reported previously.18 TLIs were calculated for the median nerves as follows: TLI=terminal distance (mm)/[MNCV (ms)×distal motor latency (ms)].
Statistical analyses
The statistical analyses were performed using SPSS for Windows, Ver. 11.0 (SPSS, Chicago, IL, USA). Percentages and means were compared by the chi-square test and Student's t-test, respectively. Correlations were determined using Pearson's correlation coefficient (r), and probability values of p<0.05 were considered to be indicative of statistical significance.
Results
Clinical manifestations
The mean age at examination was 36.9 years (range, 5-75 ye-ars) and the mean age at onset was 15.5 years (range, 2-45 years). The mean disease duration at the time of examination was 22.3 years (range, 0-57 years). The disease had manifested before the second decade of life in 69% of the patients. Twelve individuals (7%) with PMP22 duplication did not complain of any clinical symptoms. Muscle weakness and atrophy started predominantly in the distal legs, with these symptoms being noted to a lesser extent in the distal upper limbs. The paresis in the distal regions of the lower limbs varied from asymptomatic to severe weakness. Pinprick sensory loss was found in 87 (52%) patients, and proprioception loss was found in 112 (67%). The mean FDS score was 2.0 and the mean CMTNS was 11.0. Heel gait defects occurred more commonly than toe gait defects (p<0.001), and high-arched foot deformities were common (89%).
Electrophysiological findings
Both the MNCV and SNCV of the median nerve were uniformly reduced in the CMT1A patients. The CMAP of the median nerve was significantly correlated with the disease duration (Fig. 1A; p<0.001) and the CMAP of the ulnar nerve (Fig. 1B; p<0.01). However, no correlations were found between the age at onset and the CMAPs in the median and ulnar nerves (Fig. 1C, D). The TLIs were distributed over a narrow range of values.
The TLI of the patients' median nerve (0.31±0.10, mean±SD; range, 0.13-0.72) did not differ significantly from the normal values seen in healthy control subjects (0.31±0.04; range, 0.23-0.43). These results suggest that demyelination in CMT1A patients is uniformly distributed between the proximal and distal portions of the nerves.
Comparison between the mild CMTNS group and the moderate or severe CMTNS group
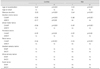
The characteristics of the mild (0<CMTNS≤10) and the moderate or severe (CMTNS≥11) CMTNS groups are listed in Table 1. The gender ratio was similar in the two groups, and the mean age at onset did not differ significantly between them. However, the disease duration at the time of examination was significantly longer in the moderate or severe CMTNS group (p<0.001). The patients in the moderate or severe CMTNS group were more severely affected than those of the mild CMTNS group by muscle weakness (p<0.001), muscle atrophy (p<0.001), sensory loss (p<0.001), the frequency of areflexia (upper, p<0.001; lower, p<0.01), heel and toe gait defects (p<0.001), and foot deformity (p<0.05). The amplitudes of the evoked median nerve motor responses were more severely affected in the moderate or severe CMTNS group than in the mild CMTNS group. In contrast, neither the MNCVs nor the SNCVs differed significantly between the two groups.
Correlation between disabilities and electrophysiological values
The CMAPs of the median (p<0.001), ulnar (p<0.001), peroneal (p<0.05), and tibial (p<0.001) nerves were significantly correlated with the CMTNS, and the CMAPs of the median (p<0.001), ulnar (p<0.001), peroneal (p<0.05), and tibial (p<0.001) nerves were correlated with the FDS score (Table 2). In contrast, the MNCV of the median nerve was only correlated with the CMTNS (p<0.05). The SNAPs and SNCVs of the median, ulnar, and sural nerves were not correlated with the disability scores.
Discussion
The present study investigated the correlations between disease disabilities and the electrophysiological findings in Korean CMT1A patients with PMP22 duplication, and found that the disabilities were related to the CMAPs rather than to the NCVs. It has been reported that CMT symptoms progress due to axonal degeneration and loss,5,19 with axonal loss being the major cause of impairment and disability in patients with CMT1A.20 The accentuation of muscle wasting and sensory impairment in the distal extremities was correlated with the corresponding reduction in the CMAPs and SNAPs but not with the decrease in MNCV or SNCV.10-12 Our results support the hypothesis that the disease-related disabilities are correlated with the decreased nerve action potentials rather than the conduction velocities.
It is important to determine how the demyelination of Sch-wann cells causes axonal injury, but this remains elusive.21 Many hypotheses have been postulated.22-25 For example, local biochemical changes in axons, such as decreased neurofilament phosphorylation, increased neurofilament density, and decreased axonal transport due to demyelinating Schwann cells, could lead to axonal dysfunction and eventual axonal loss.9 Some longitudinal CMT studies have revealed that nerve conduction velocities remain unchanged for more than 10 years, but that the CMAPs progressively decrease over the same period.16,26 In the present study we also found an absence of velocity changes over a 10-year period in nine patients despite gradually increasing clinical severities. These results suggest that the degree of change in CMAP amplitude is useful for predicting the clinical severity of the disease. As a marker of axonal loss, the reduction in CMAP amplitude appears to be more closely linked with the disability. We also found that the clinical manifestations of muscle atrophy were also strongly correlated with the CMAPs and axonal loss, which became more pronounced as the disease progressed.
The disease severity varies considerably among patients with CMT1A.27 Attempts to identify the mitigating factors are underway, and these efforts could lead to effective therapeutic approaches for reducing the expression of PMP22.28 PMP22 duplication mainly induces a demyelinating phenotype, while the features of axonal pathology appear concomitantly with advancing age.6 The patients with PMP22 duplication show a great variability of disease severity, ranging from asymptomatic individuals to wheelchair-bound patients. These results suggest that other molecular, endogenous, and environmental factors (e.g., genetic factors related to the PMP22 expression) influence the progression of this disease.
In the present study, the age at onset was the first decade in 44% of the CMT1A patients and before 20 years of age in 69%. The age at onset as an indicator of the CMT disease severity has been the subject of debate.11,12,26 Although Birouk et al.13 reported an association between the age at onset and the severity of the disorder, others have suggested that the age at onset is not a reliable indicator of disease severity; the latter is consistent with our findings.11,26 Instead, one of the most important disease-modifying factors in our study appeared to be the disease duration. A longitudinal study found that axonal involvement progressed in a time-dependent manner, and that axonal degeneration proceeded concomitantly with advancing disease.10,16 The age-dependent reduction in the CMAPs, and the increase in axonal degeneration and clinical disability observed in our study were also in good agreement with previous reports.15,29 Furthermore, the median nerve TLI did not differ between Korean CMT1A patients and healthy controls. Despite the distal location of the CMT symptoms, the nerve conduction velocities slowed uniformly along the proximal and distal segments, which implies a uniform pathological process of demyelination.
In conclusion, a significant correlation was found between the clinical-electrophysiological manifestations and the physical disabilities among the Korean CMT1A patients in this study. Although our study was cross-sectional in design and involved only a single race, we propose that the clinical disease severity in patients with CMT1A is determined by the extent of axonal dysfunction.


 XML Download
XML Download